- Decreased RMP
- Velocity (Vmax) of Ph 0 decreases as RMP becomes less negative
- Threshold potential decreases (from -75mV to -70mV)
- Increase in slope of Ph 2 & 3 shortening repolarisation time (responsible for ST-T depression, peaked Tw & QT shortening)
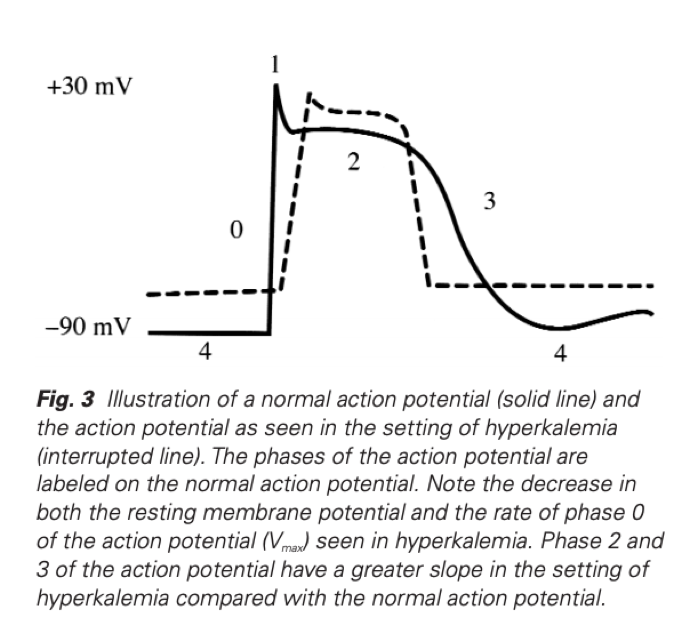 Hyperkalaemia Revisited, Parham W et al, Tex Heart Inst J 2006;33:40-7
Hyperkalaemia Revisited, Parham W et al, Tex Heart Inst J 2006;33:40-7 
This qn was recalled as something in regards to a defibrillator capacitance refers to…
Capacitance is the ability to store charge (SI = Farad)
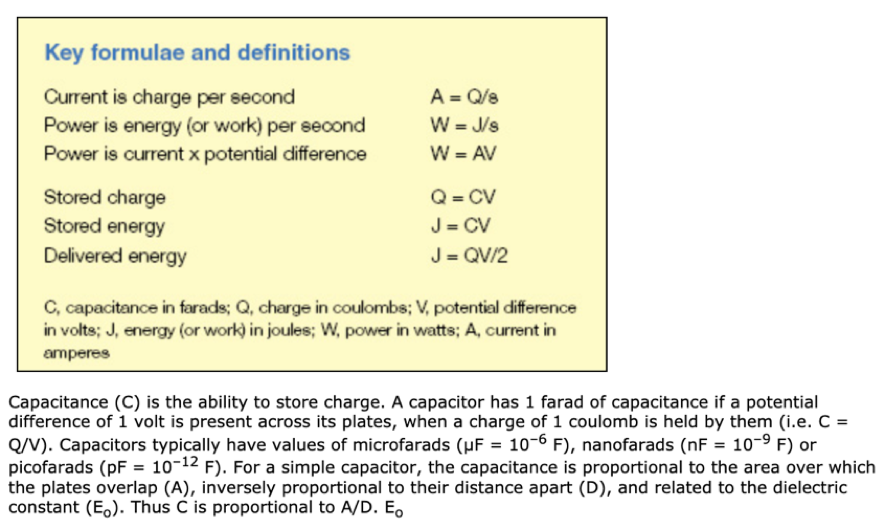
An additional variable added to the 2019 MCQ

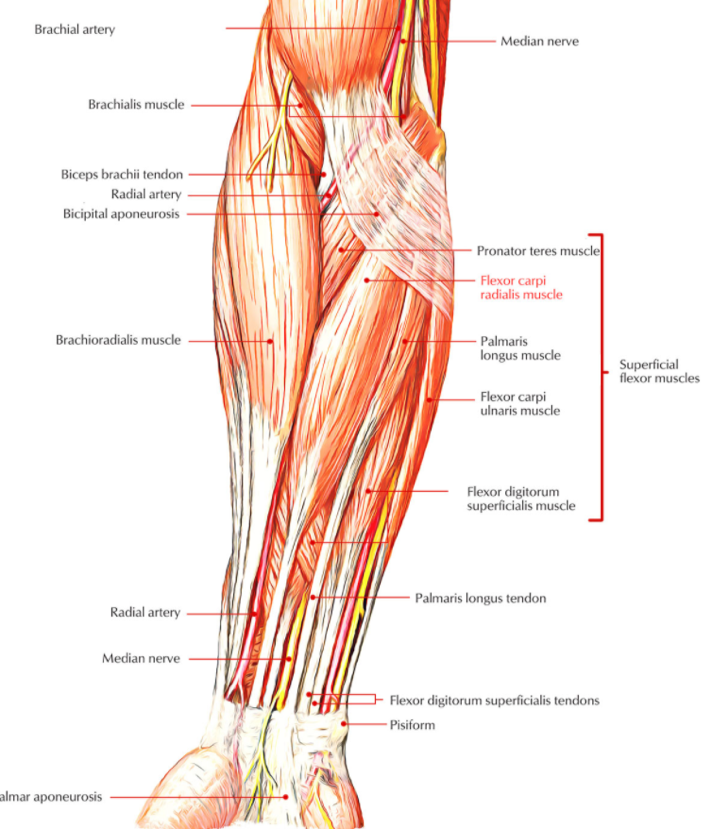
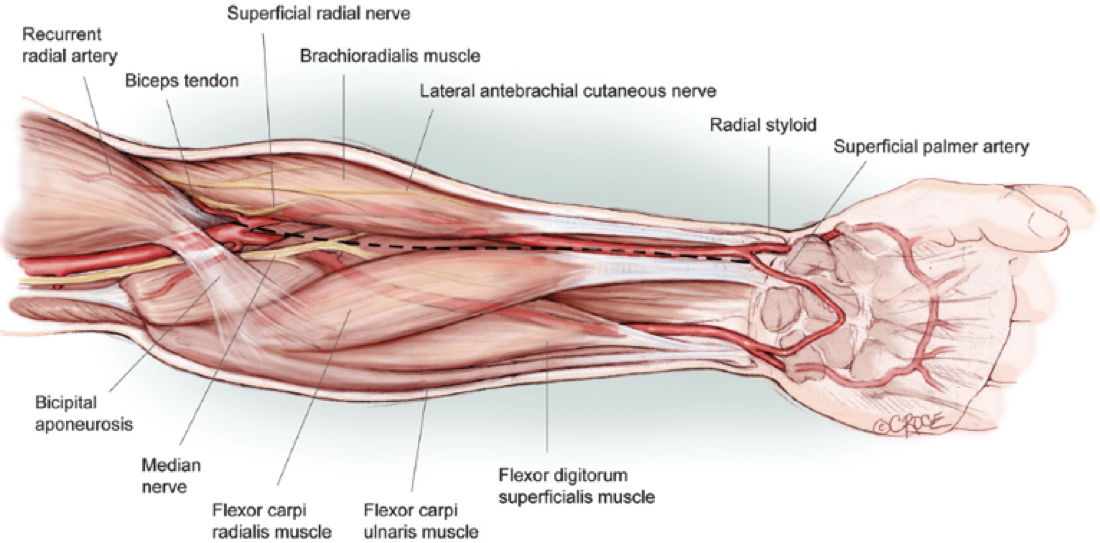 Harvesting the Radial Artery
Arie Blitz et al
Harvesting the Radial Artery
Arie Blitz et al 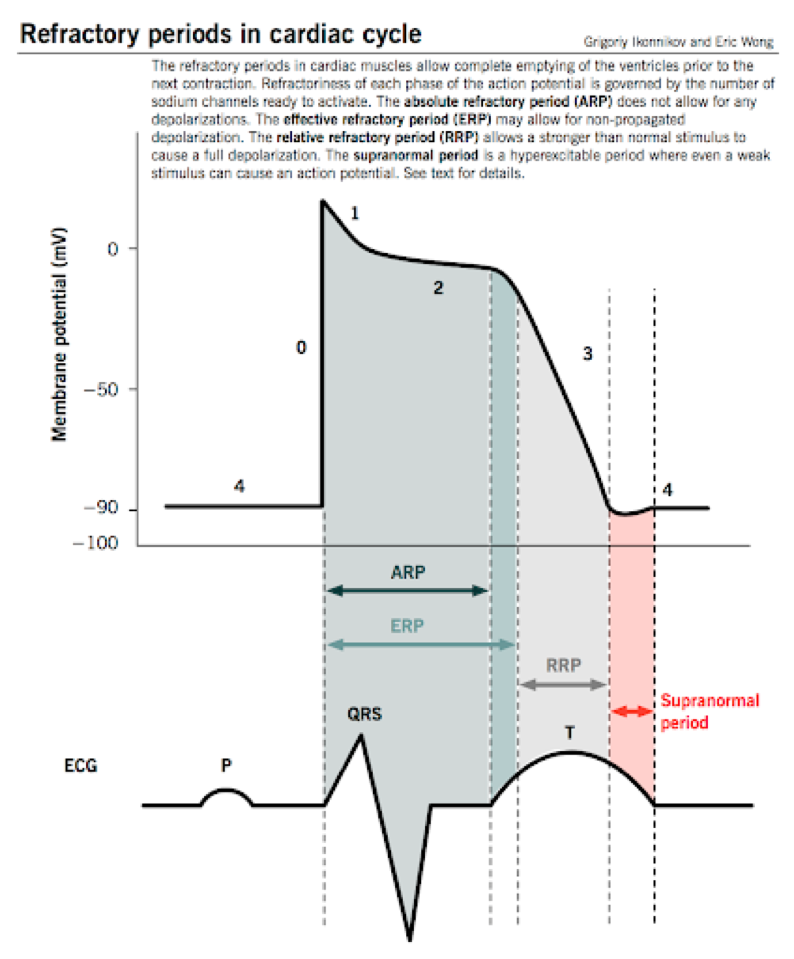 Isovolumetric ventricular contraction
Isovolumetric ventricular contraction
- The beginning of this phase corresponds with the peak of the R wave
- This corresponds to Phase 0 (rapid sodium influx) of the ventricular myocyte action potential
- The ventricles begin to contract during this period
- This contraction increases the ventricular chamber pressure and closes the mitral and tricuspid valves.
- As a result, there is a fixed ventricular volume during this contraction
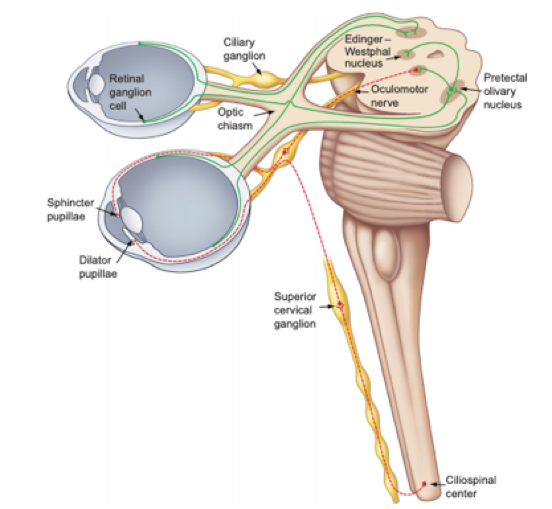
- Olivary Pretectal Nucleus
- Edinger Westphal nucleus
- Ciliary Ganglion
- Contralateral Pretectal Nucleus
 Deranged Physiology
Deranged Physiology