A cardiac glycoside naturally occurring in many plants
Glycose → glucose → required to fixate the glycoside to cardiac muscle
Aglycone → influences PD effects
Load: IV 0.5mg/30mins or 10mcg/kg
Maintenance: 0.125 – 1mg/day
PO/IV
IV: 15 mins
PO: 1 – 6hrs
Several days
t ½ 40hrs with normal renal function
Peripheral vascular effect
Myocardial → DIRECT → MECHANICAL
Myocardial → DIRECT → ELECTRICAL
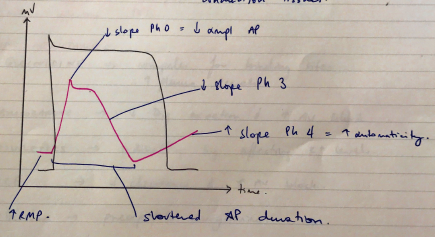
= ↑automaticity
Myocardial → INDIRECT → ↑PARASYMP ACTIVITY
→ CHOLINERGIC INNERVATION MORE PRONOUNCED IN ATRIA →
∴ affect atria & AV node movement
Peripheral vascular effects
Prolonged PR
Delayed AV conduction
Scooped out ST
↓slope Ph 3 due to ↑K conductance
T waves ↓amplitude ST inversion
Shortened QT
↑K conductance, shortens AP
NO EFFECT QRS DURATION
Because digoxin doesn’t alter conduction through ventricles or conduction tissues
CVS
RENAL: ↑renal perfusion & mild diuresis
Elderly: ↓skeletal m. = ↓reservoir = ↑plasma levels
Renal failure: ↓dose
Ab development: ↓therapeutic effect
ANTIARRHYTHMICS
75% OBA
Peak plasma in 1 – 2hr
PPB 25%
VD 6L/kg
Tissue affinities:
→ Principle reservoir
Minimal
Excreted by kidneys unchanged
Depends on CrCl
t ½ B = 2 days!
NOT REMOVED BY DIALYSIS
[Digoxin] myocardium = much more than plasma
Monitor levels
→ 6 – 12hr post dose
→ 0.6 – 2.6nmol/L
But relationship between level & pharmacological effect not always consistent
→ <0.5nmol/L = no dig toxicity
→ >3nmol/L = definitely toxic
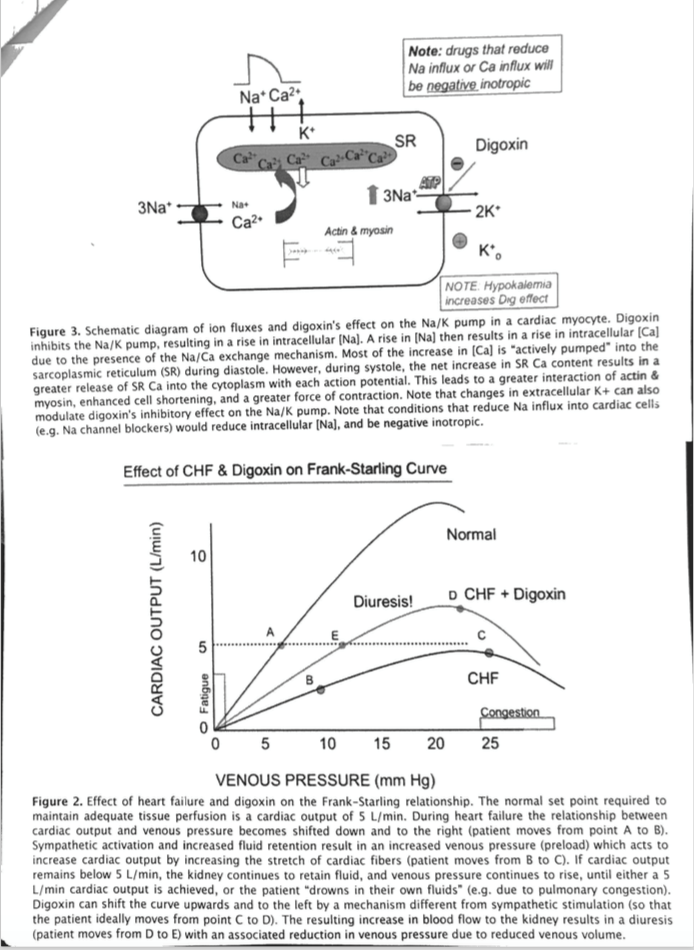
TOXIC EFFECTS → Na/K/ATPase inhibition
CNS
GI: anorexia, N&V (stimulations CTZ)
RISK FACTORS:
Tx:
→ Bind dig ∴ less available to inhibit Na/K/ATPase
→ Dig-Ab complex eliminated by kidneys