The term comes from the French ‘tonka bean’ = COUMAROU, from where coumarin was first isolated
Use
Prevent emboli in AF, value disease, prosthetic valves
Tx DVT/PE
Presentation
Oral tablets 1 – 10mg
Racemix mixture
S-isomer x 4 potent
Dose / Route
5 – 10mg OD orally for 3 days
→ Daily bloods
→ Then alternate days for 1/52
→ Then fortnightly
Dose/route overlap for a minimum of 5 days, until target INR has been reached for at least two consecutive days (Pisters et al. 2010; Rossi 2015).
Because of the shorter half life of protein C and S they drop prior to the clotting factors and as such warfarin can produce an pro-thrombotic phenotype in the first few days
Target INR
AF 2 – 2.5
Prosthetic valve 2.5 – 3.5
All else 2 – 3
Onset
8 – 12hrs onset
Warfarin halts production of new clotting factors
No effect on already active factors
∴requires hours for full effect (for all of those factors to be degraded) → mainly F II (PRO THROMBIN)
DoA
Half lives:
of Protein C/s → 7 → 9 → 10 → 2
= 7 6 24 40 60hrs
DoA → effects last 2 – 5 days (life of clotting factors)
Very slow clearance 3mL/kg/min & new clotting factors need to be synthesised
MoA (mechanism)
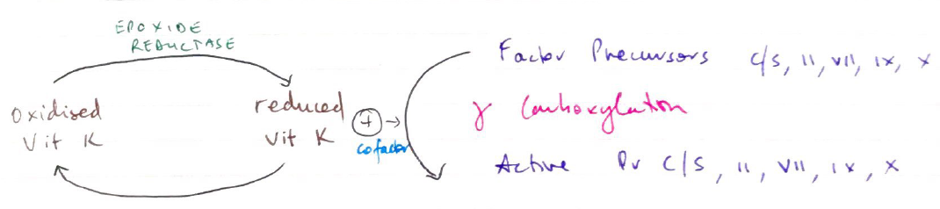
Inhibits production of Vit K dependent clotting factors & proteins
Vit K is required to synthesise:
4 clotting factors: II, VII, IX, X (TV channels)
2 anticoag proteins; Pr C & S
Formation of these requires y-CARBOXYLATION
Reduced Vit K (as cofactor)
Warfarin inhibits EPOXIDE REDUCTASE. This enzyme reduces oxidised Vit K so it may be used again
∴ no cofactor for carboxylation → ↓ synthesis clotting factor & protein