An acetanilide derivative
1g QID
PO/PR/IV
Antipyretic
Analgesia
CNS
High lipid solubility
Rapid absorption
OBA 60 – 90%
More PR (OBA)
pKa 9.5 (weak acid)
<1% PPB
Highly UNIONISED at pH 7.4
Lipid soluble
Penetrates BBB +++
VD 1L/kg
HER 0.3
80% to glucuronide & sulphate
10% to NAPGI via CYP450 which is then conjugated with glutathione
<5% unchanged in urine
Metabolites actively secreted into renal tubules
t ½ B 2 – 4hrs
PARACETAMOL TOXICITY
Toxicity = the degree to which something is poisonous
Metabolised by 2 pathways
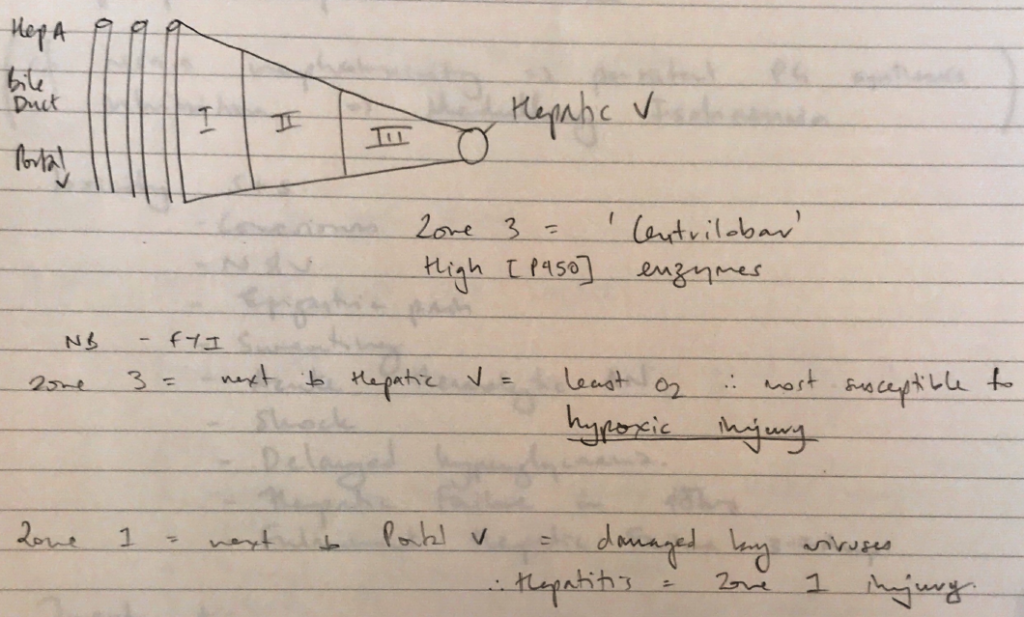
Mechanism of toxicity
4 mechanisms of liver damage
When NAPQI reacts with hepatocytes = IRREVERSIBLE INJURY
Nephrotoxicity
Cf. NSAID nephrotoxicity → persistent PG synthesis inhibition → medullary ischaemia
Toxicity S+S
TREATMENT