H3i / 20A14 / 19A18: Describe the pharmacology of frusemide
20A14: Exam Report
Describe the pharmacology of frusemide.
51% of candidates passed this question.
Most candidates presented a well-structured answer and provided a basic understanding. Answers that provided accurate indications and details of the mechanism underlying the actions of frusemide attracted more marks. Those recognising the increased delivery of sodium and chloride to the distal tubule (exceeding resorptive capacity) were awarded more marks that those answers that attributed the diuretic action solely to reduction in the medullary gradient. Frusemide has many potential adverse effects and a reasonable list was expected. Conflicting information was common (e.g. highly bound to albumin – Vd 4 L/kg) and better answers avoided this.
19A18: Exam Report
Describe the pharmacology of frusemide.
13% of candidates passed this question.
The majority of answers were well structured, some using tables and others using key headings. In general, for a commonly used drug that is listed in the syllabus as Level 1 of understanding, detailed information was lacking. In particular, mechanism of action, dose threshold and ceiling effect and pharmacokinetics lacked detail and/or accuracy.
H3i / 20A14 / 19A18: Describe the pharmacology of frusemide
Chemical
LOOP diuretic
Use
- Oedema
- Renal impairment
- HTN
- ↑ICP
Presentatation
Photosensitive solution (brown ampoules) 10mg/mL
20/40/500mg tabs
Dose
Threshold Dose
No diuretic effect when dose is lower than threshold dose
Dose-responsive effect
Threshold dose depends on clinical condition
Normal renal fn; 10mg = threshold dose
Advanced CKD <80mg below threshold
Ceiling Dose
Dose at which there is maximal sodium excretion
Dose-responsive effect, but above ceiling dose there is little diuretic effect
Frusemide will decrease preL → decrease CO → ceiling is the level of diuresis where there is no scope for preL to decrease any further
Repeated infusions w ceiling dose are more effective than increasing dose
Ceiling dose varies w different diseases
ie 40-80mg CCF, liver cirrhosis
80-200mg CKD, nephrotic syndrome
MoA
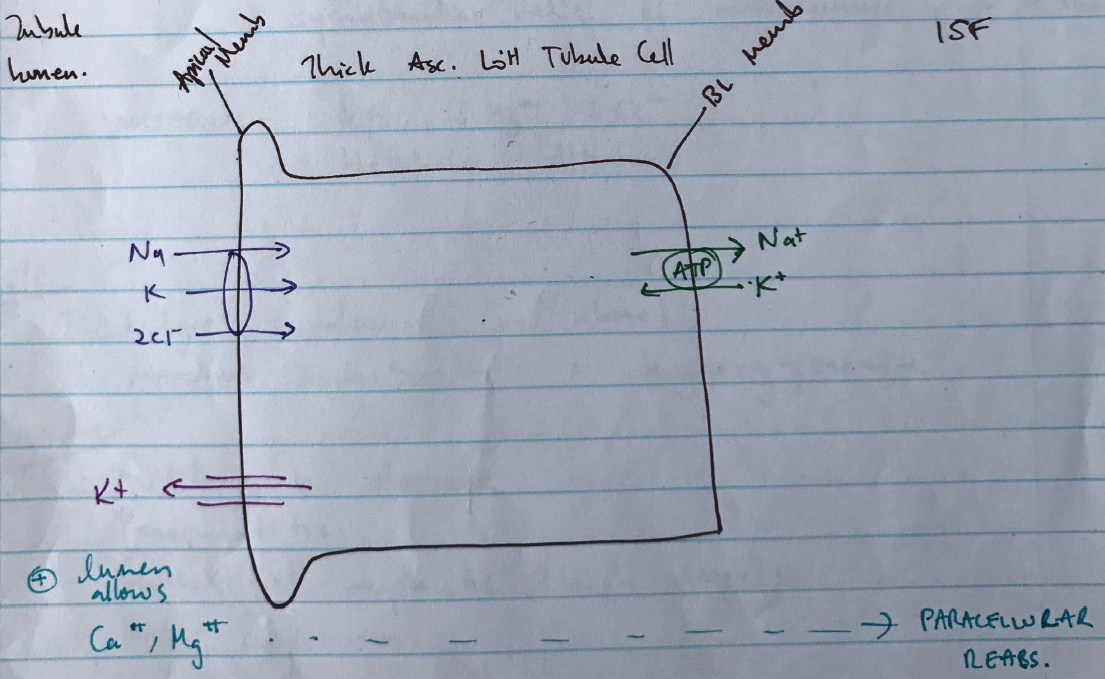
- Inhibits Na/K/2Cl transporter on Thick Asc. LoH
- Most potent diuretic
- 25% filtered Na+ not reabsorbed, thus increased presentation of solute to distal tubule
- Potent diuresis
- Late in tubule ∴ minimal compensation
- Loss of counter-current multiplier of medulla nephrons
- Loss of K+ recycling generating +ve luminal voltage
- ∴loss of Mg2+ & Ca2+
PD
Renal
- Diuresis
- ↑RBF
- ↓O2 consumption of LoH
CVS
- Pulm & systemic VD = symptomatic relief of breathlessness prior to diuresis
Metabolic
- ↓K, ↓Mg2+, ↓Ca2+
- Metabolic alkalosis
PK
A
60 – 70%
D
96% PPB
VD 0.1L/kg
M
Renal to glucuronide
E
80% in urine unchanged
Glucuronated frusemide
Faecal
t ½ 45 – 90mins
A/E
- Electrolyte imbalances (see below)
- ↓insulin sensitivity = hyperglycaemia
Toxicity
- Auditory n. damage
- Pancreatitis
- Interstitial nephritis (high doses)
- BM depression
Special: Electrolyte Imbalances
Hyponatraemia & Hypochloraemia
- Loop diuretics excrete 25% filtered Na+ load
- Inhibit Na/K/2Cl symporter
- Very late in nephron ∴little chance to reabsorb
- ∴significant Na+ & Cl– loss
Hypokalaemia
- Inhibits Na/K/2Cl symporter
- ↓Na & H2O reabsorption
- ↑[Na] reaching DCT & collecting duct
- At DCT & collecting duct more Na+ reabsorption cf. Cl–
- Leaves negative voltage in lumen
- Attracts K+ & H+ → lost in urine
- Any diuretic given proximally to K+ secretory site (DCT, collecting duct)
- ↑Na & H2O loss = ↑tubular flow
- ∴↑K+ secretion
- ↓ ECF volume
- Stimulates aldosterone
- Promotes K+ excretion
Hypocalcaemia & Hypomagnesaemia
- Due to altering voltage
- Normally the Na/K/2Cl pump requires K+ recycling
- Creating a positive voltage in Thick LoH
- This promotes paracellular reabsorption of Mg2+ & Ca2+
- Inhibiting Na/K/2Cl negates K+ recycling
- ∴loss of positive voltage & loss of Ca2+ + Mg+ reabsorption
Metabolic Alkalosis
- ↓ECF volume due to Na+ not being reabsorbed
- Subsequent ↑Na+ reabsorption at PCT
- ↑Na+/H+ antiporter activity
- Causing maximal HCO3– reabsorption at PCT (almost all)
- ↓ECF volume
- ↑aldosterone
- ↑H+ secretion by Principle Cells
- Because almost all HCO3– loss has been reabsorbed at PCT
- H+ secretion is with non HCO3– buffer → which generates new HCO3–
- Hypochloraemia
- ↑SID
- Alkalosis
- Diuresis = Na, H2O, Cl loss
- Cl & HCO3– = main ANIONS of ECF
- ∴loss of one = ↑reabsorption of other to maintain ELECTRONEUTRALITY
- ∴↑HCO3–
→ Correction in vol will not correct metabolic alkalosis → you need to correct Cl– deficit with 0.9% NaCl
→ Overall METABOLIC ALKALOSIS
Hyperuricaemia
- Dose-dependent, drug-induced GOUT
- ↓urate excretion by
- ↑Urate reabsorption
- ↓Urate secretion
- PCT = main site of urate handling
- Most filtered urate is reabsorbed
- Loop diuretics amplify PCT reabsorption of urate
- ↓ ECF = ↑aldosterone, ↑urea reabsorption
- OVERALL → hyperuricaemia
Hyperglycaemia
- Impairs insulin sensitivity