A methylxanthine derivative
Tx bronchoconstriction
Tablet, syrup, solution for IV injection
Loading Dose 7mg/kg calculated by IB and given over 30 minutes
Maintenance 0.6mg/kg/hr (IV) or 7mg/kg (PO)
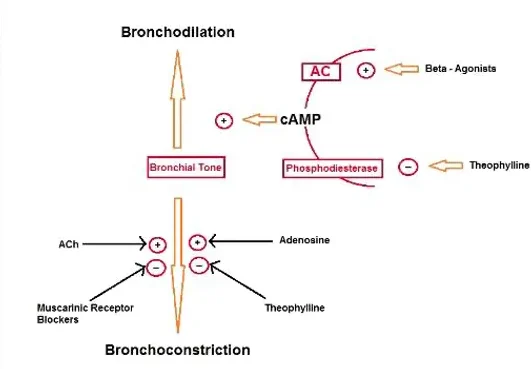
PHOSPHODIESTERASE INHIBITOR
ADENOSINE RECEPTOR BLOCKER
Resp
CVS
GU
Bronchodilation occurs over a concentration of 5-20mcg/ml
As concentrations >20mcg/ml so do the frequency & severity of adverse events
Metabolic
CNS
MSK
P50 interactions