Cardiac defects → R – L shunt (true mixed venous blood)
NOTE: Although bronchial & thebesian veins do not contain true mixed venous blood (&∴ strictly can’t be calculate with SHUNT EQUATION), we do use shunt equation to quantify them
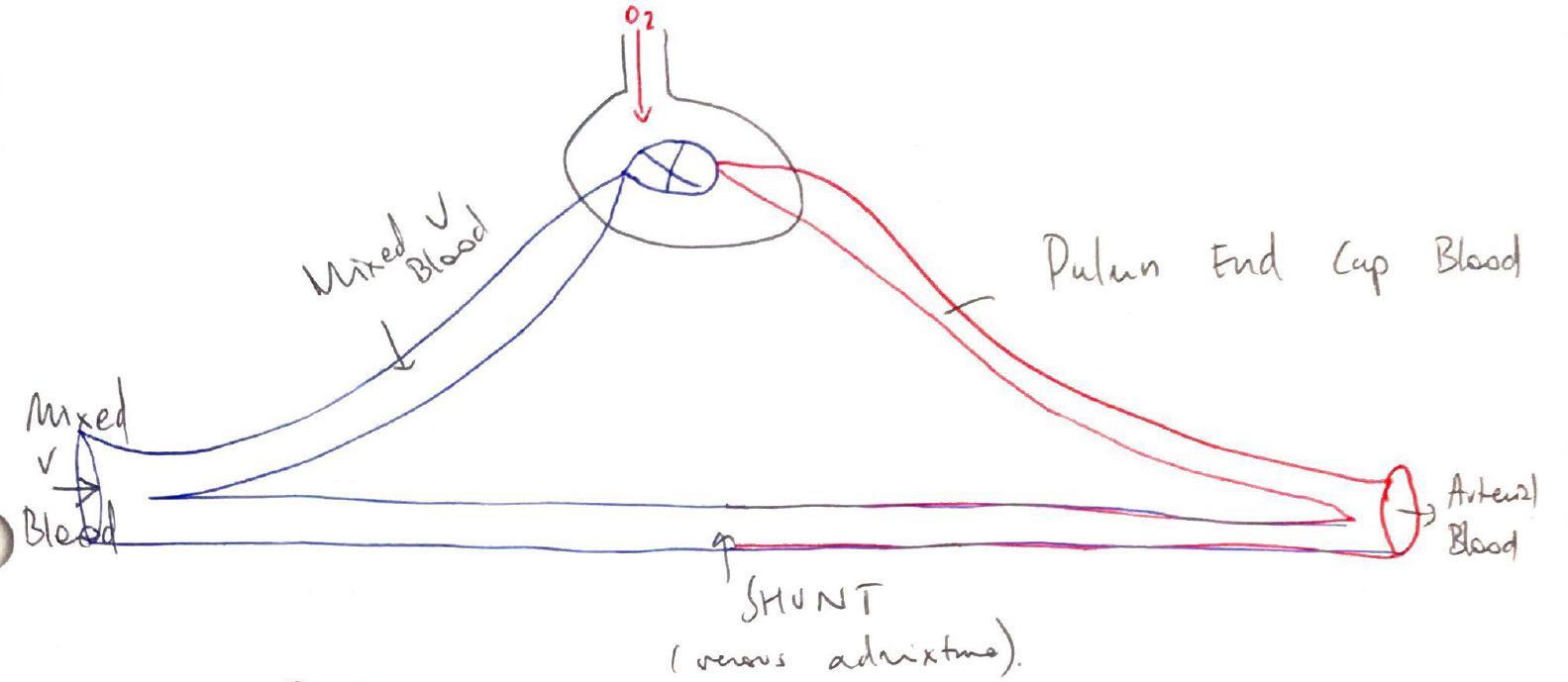
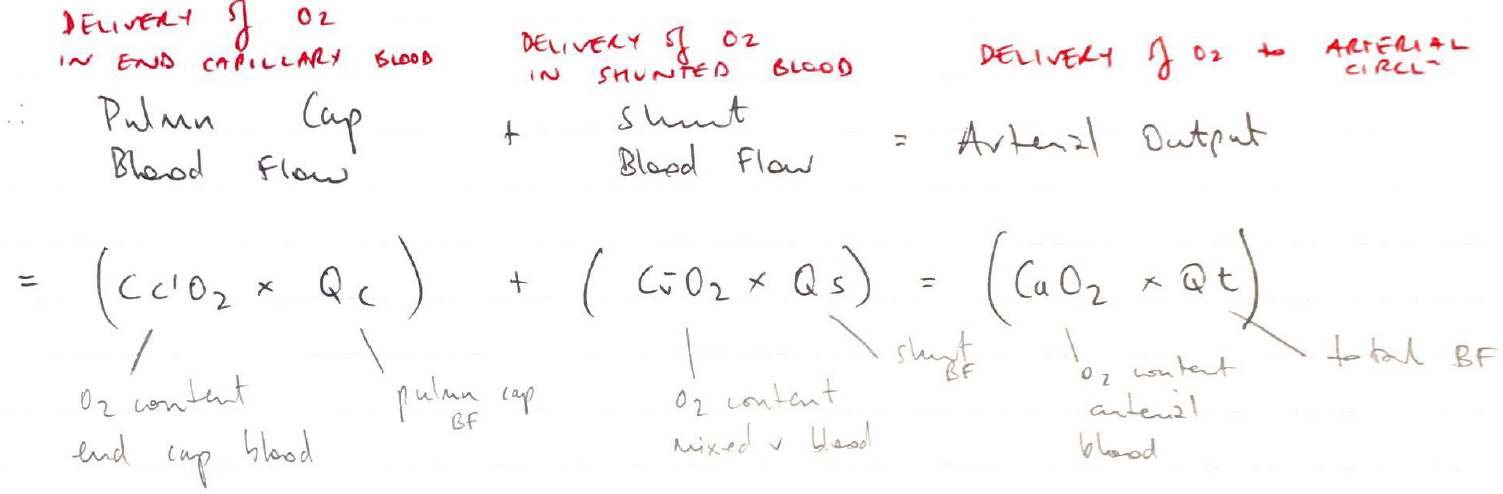
Quantifying Shunt = Shunt Equation
Normally expressed as % → 2 – 3%
If Cc’O2 = 20mL/dL and CvO2 = 10mL/dL:
∴50% shunting will give CaO2 = 15mL/dL
∴25% shunting will give CaO2 = 17.5mL/dL
Effect of Shunt on PO2
Shunt ↓O2 content of arterial blood
This does not respond to ↑FiO2
Because no matter how much ↑FiO2 you give, the shunted blood is never exposed to it
∴giving 100% FiO2 is a useful diagnostic test → there’s a huge A – a gradient
The larger the shunt, the smaller the ↑PaO2 for given ↑FiO2
Sigmoid ODC:
Blood passing past high FiO2 units is already fully saturated its Hb, so any additional O2 is only dissolved, which is small
Blood coming out of these units is not enough to close the shunt gap
Effect of Shunt on PCO2
Shunted blood does not ↑PaCO2
2 reasons:
CO2 curve is linear → regardless if PO2 is high/low
Respiratory compensation
Any ↑PaCO2 stimulates chemoR → ↑MV
Keeps PaCO2 normal range
This ↑MV does not connect hypoxaemia
But hypoxaemia can ↑MV further (so PaCO2 may even be low)