This question was best answered through a description of how the entire nephron excretes acid.
This required a detailed description of bicarbonate reabsorption, ammonium excretion and titratable acidity including phosphate.
Explanations were expected to describe the locations, cells and the mechanisms or transporters involved in the resorption of bicarbonate or excretion of acid and how these changes depending on acid load.
20B19: Exam Report
Explain how the kidney handles an acid load
51% of candidates passed this question.
This question required candidates to understand the renal response to an acid load. It was expected that candidates would answer with regard to recycling of bicarbonate in the proximal tubule, excretion of titratable acid via the phosphate buffer system and generation of ammonium and its role in acid secretion. Many candidates had a good understanding of the bicarbonate system but used this to explain the secretion of new acid.
14B12: Exam Report
Describe the role of the kidneys in the excretion of non-volatile acid.
27% of candidates passed this question.
This is a complex but essential area of physiology for intensive care practice. It was expected candidates would indicate that non-volatile acids are those not able to eliminated by the lungs (lactate, sulphate, phosphate and ketone bodies). The kidney plays a central role via bicarbonate (resorbing filtered bicarbonate and generating “new” bicarbonate = acid excretion). It was expected candidates could detail the processes in various parts of the renal tubules and the role or urinary buffers (dibasic phosphate and ammonia).
While a number of candidates were able to provide some of the details of ion transports in the kidney, few showed understanding of the overarching concepts of the proximal bicarbonate reabsorption being necessary to allow the distal acid excretion.
H1v / 24B14 / 20B19 / 14B12: Describe the role of the kidneys in the excretion of non-volatile acid
Definition
Non-volatile acid: an acid not excreted by lungs
Fixed acid production = 1 mmol / kg / day
Due to incomplete metabolism of:
Carbohydrates → lactate → 1500 mmol/day
Protein → sulphate, phosphate → 55 mmol/day
Fat → ketones → 12 mmol/day
These acids require excretion by the kidneys for acid-base balance (~70 mmol/day)
NB: lactic acid is exempt because 1500mmol of lactic acid produced is oxidised by the liver to regenerate HCO3–
Kidney has 2 important roles in acid-base & excretion of fixed acids
Reabsorb all filtered HCO3–(4320 mol/day)
Excrete fixed acids (70 mmol/day)
1) HCO3- Reabsorption
Daily acid load cannot be excreted unless all filtered HCO3– is reabsorbed
Because both derived from H2CO3 dissociation
H2CO3⮂ H+ + HCO3–
Losing HCO3– is like gaining H+
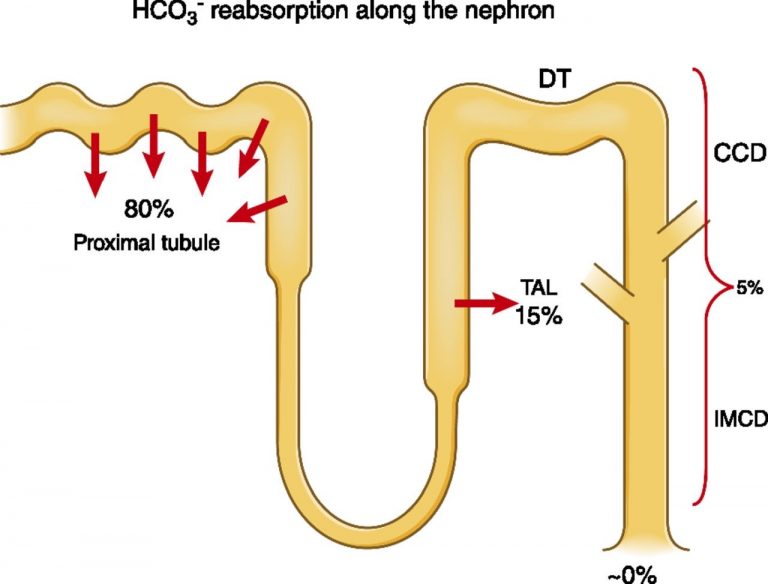
HCO3– reabsorption
80% PCT
15% thick ascending LoH
Rest Type A intercalated cells of Collecting Duct
Plasma HCO3– = 24mmol/L
GFR = 180L/d
∴Filtered HCO3– = 4320 mmol/day
HCO3– reabsorption is active
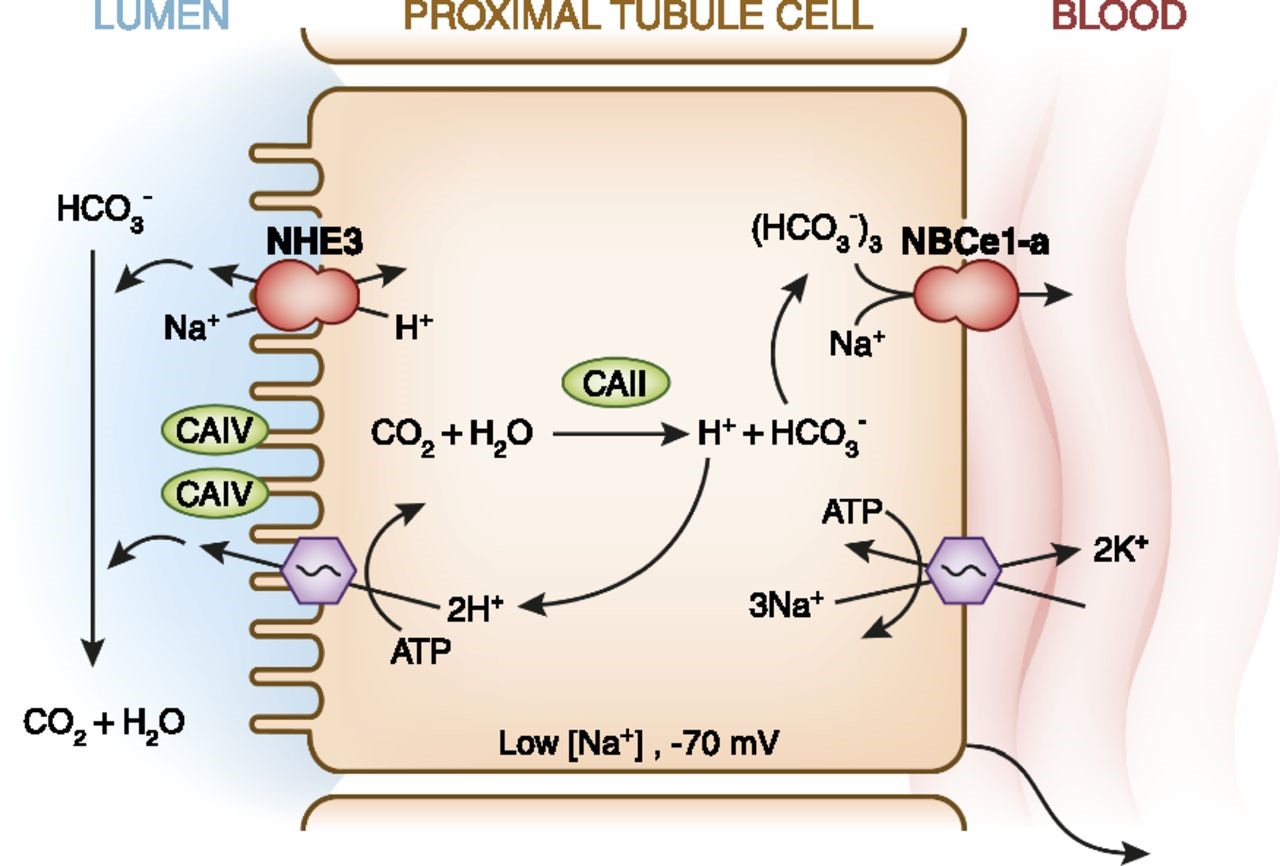
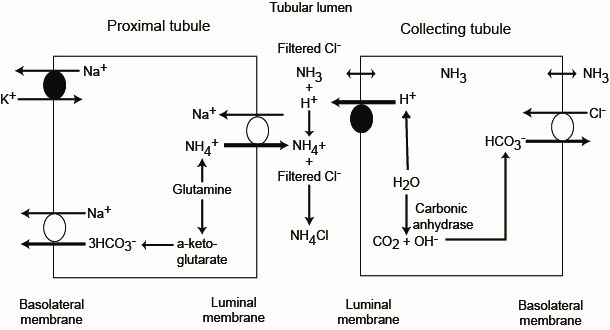
PCT
CA present on apical membrane & inside tubule cells
Catalyse: CO2 + H2O ⮂ H2CO3 ⮂ H+ + HCO3–
HCO3– produced inside tubule cell is reabsorbed across BL membrane → peritubular caps
H+ crosses apical membrane → CO2 + H2O
∴H+ is not added to urine → forms H2O with CA enzyme on apical membrane
Transporters Required
Na/K/ATPase BL membrane to reabsorption Na+
Na/3HCO3– – symporter BL membrane to reabsorb HCO3–
Na/H antiporter apical membrane to secrete H+(Bonus – reabsorbs Na+!)
Thick Ascending LoH
Reabsorbs 15% HCO3– filtered
Similar to PCT
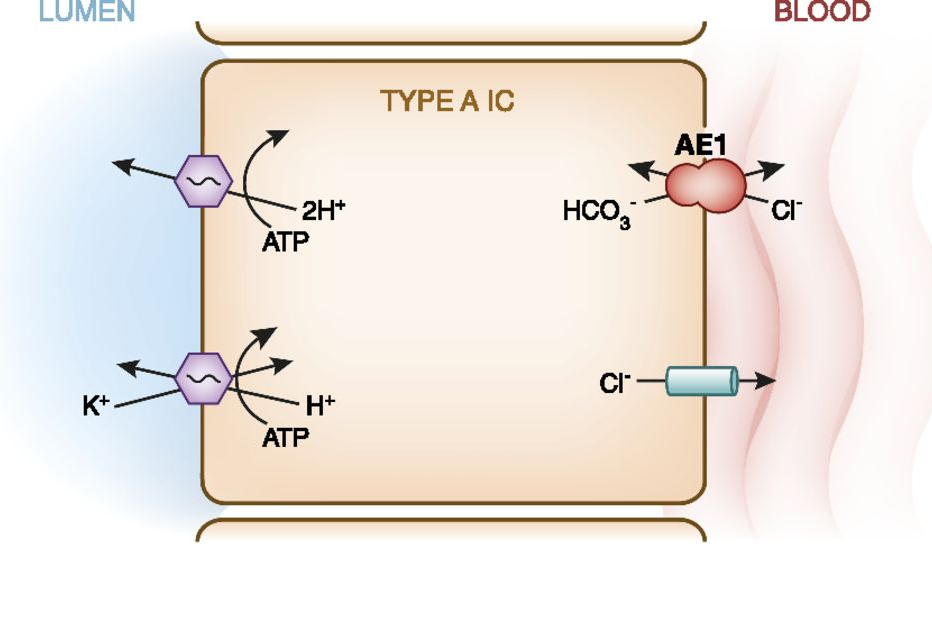
DCT/Collecting Ducts
Type A Intercalated Cells
Secrete H+ to form titratable acid & reabsorb HCO3–
Transporters
H/ATPase
H/K/ATPase (↑ with aldosterone)
Cl/HCO3– symporter
2) Fixed Acid Excretion
Requires new HCO3–to be formed
Difficult to excrete free H+because its urine concentration is so low < 0.04mol/L even at the most acidic pH
Fixed acid = 70 mmol/day
2 buffer system in URINE
AMMONIA → excretes 50 mol
PHOSPHATE → excretes 20 mol
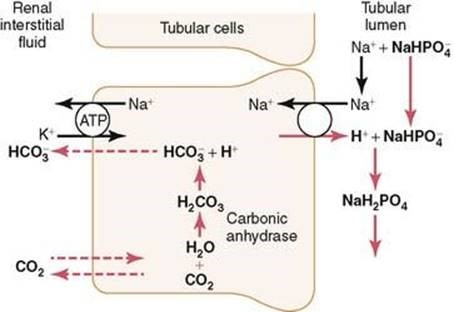
Phosphate buffer system
H2PO4(weak acid) ⮂ H+ + HPO42-
H2PO4– is the “titratable acid” & refers to the amount of NaOH required to titrate the urine to pH 7.4 (which must equal the amount of H+ mol in urine)
NH4+ is not part of titratable acidity. pKa 9.2
∴ exists as NH4+ & does not dissociate in urine
∴ doesn’t contribute to urinary pH (& ∴ not measured w titration)
NB: To measure, you need to measure urinary NH4+
Phosphate Buffer
= pKa 6.8
Occurs in late DCT & collecting duct
H+ secreted into tubule lumen & binds HPO42-
To reach min. tubule pH 4.4
Note on Phosphate
Plasma phosphate = 1 mmol/L
90% free, rest bound to plasma proteins
GFR 180L / day ~160 mol /day filtered phosphate
~90% reabsorbed
∴ ~40 mol/day un-reabsorbed H2PO4– available for buffering
BUT
This system cannot be upregulated with ↑ acid load
At pH 7.4 80% base HPO42- and 20% weak acid H2PO4–
But as tubule fluid pH ↓, most is converted to acid H2PO4–
Ammonium Buffer = pKa 9
In PCT cells extract glutamine from GFR & peritubular capsule
Glutamine → 2NH4+ + 2HCO3–
Na/NH4 antiporter secretes NH4+ into tubule fluid
HCO3– diffuses into peritubular caps
NH4+ is not lipid soluble & trapped in tubule lumen → (excreted H+)
Thick Ascending Limb
80% NH4+ reabsorbed
Na / K / 2Cl multiporter with NH4+ substituting for K+
Causes NH4+ to accumulate in interstitium of medulla
Its [ ] ↑ approaching papillar & some is secreted into Thin Desc. Limbs
This is ‘ammonium recycling’ & some trapped in medullary interstitium
Collecting Ducts
NH4+ secretion
That which is reabsorbed in Thick Asc. Limb is put back into tubule & secreted
Overall : new HCO3– reabsorbed
Other buffers contributing to titratable acidity (but not that significant):
Creatinine
pKa 4.9 → at pH 4.4 in urine can contribute to titratable acidity
B hydroxybutarate & acetoacetate
pKa 4.5 → ketoacids appear in urine during DKA. Act as buffers during severe metabolic acidosis (because the H+ will only bind with them at low urinary pH due to their pKa)