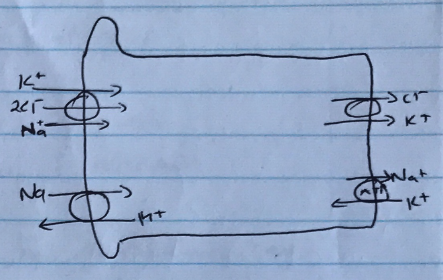
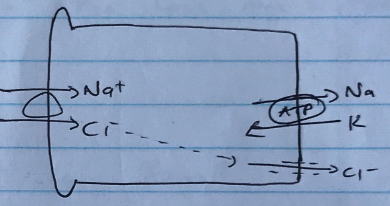
A description of filtration and reabsorption, including amounts was required. Better answers described sodium handling in a logical sequence as it progressed through the nephron including the percentages reabsorbed in each segment. In addition to the amounts reabsorbed, the mechanisms of transport across the tubular luminal and basolateral membranes into interstitial space should have been described.
H1v / 18A04: Describe the renal handling of sodiu
Definitions/Values
Sodium = major cation of ECF
Plasma level 140mmol/L
180L/day GFR → 25,000 mol Na+ filtered/day
140mmol excreted → 0.5% fractional excretion
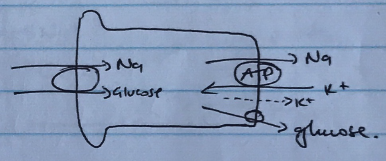
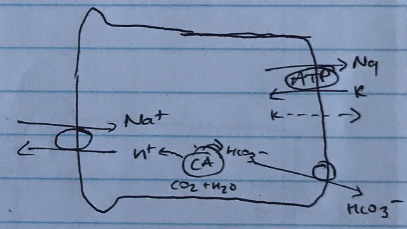
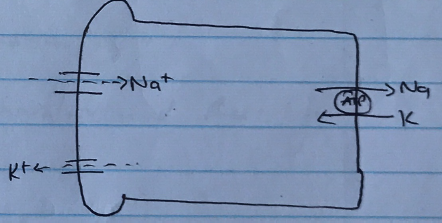
PCT
65% reabsorbed
Co-transport with nutrients (amino acids, glucose) → driven by Na/K/ATPase
Counter-transport with Na/H exchange
HCO3– reabsorbed
Driven by Na/K/ATPase
Stimulated by AII
Inhibited by Acetazolamide
Passive diffusion by SOLVENT DRAG
Late DCT favours osmosis because early PCT does major solute reabsorption
This will drive Na+ reabsorption by solvent drag with H2O