23A05: Exam Report
Describe renal handling of potassium (60% of Marks), including physiological factors that may influence it (40% of Marks)
33% of candidates passed this question.
This question related to the renal handling of potassium, the physiology of potassium in the rest of the body was not relevant. Ultimately net potassium flux is a function of filtration, reabsorption, secretion and excretion.
Good candidates divided the nephron into relevant sections and described how potassium was handled in each section. They correctly described the percentage reabsorption along each section, as well as the relevant active and passive pathways for reabsorption and/or secretion including the cells and channels/pumps involved.
The physiological factors regulating each of these mechanisms were then described in correct detail.
21A08: Exam Report
Describe renal handling of potassium (60% marks), including factors that may influence it (40% marks).
33% of candidates passed this question.
This question covers a core physiology topic. The detail required is well described in the recommended reference texts. Generally, this question was poorly answered. From an answer template perspective, a “describe question” in this context involves both the stating the relevant potassium handling mechanism and then giving a description of how it occurs and how this system is regulated. Many answers that scored poorly simply listed sites of potassium handling but excluded the details surrounding the specific
receptors and channels involved as well as the processes that exist to perpetuate and regulate these biological processes. Simple identification as to whether the potassium was being secreted or reabsorbed as well as the location as to where this may occur within the nephron, were often not specifically detailed or used interchangeably. Such answers scored poorly.
H1v / 23A05 / 21A08: Describe renal handling of potassium (60% marks), including factors that may influence it (40% marks)
- K+ is the major intraceullular cation
- Key role in RMP (regulation is vital to sustain life)
- Plasma K = 3.5-5mmol/L
Potassium is freely filtered by the kidney
Filtered load = GFR x plasma concentration (180 x 4.2mmol/L = 756 mmol/day)
It is then both reabsorbed and secreted, and regulation of body potassium occurs mainly via control of secretion.
Normal urinary K+ excretion is 20-150% of filtered K+, and can be as low as 2% with K+ depletion. This is approximately 92mmol/day.
Renal Handling
Tubular Location
% of K+ (Reabsorbed/Secreted)
Cellular Process
PCT
% of K+ (Reabsorbed/Secreted)
55% reabsorption
Cellular Process
Passively via the paracellular route due to:
- Solvent drag → coupled to flow of Na+ and H2O
- [ ] gradient → created by reabsorption of H2O
- Electrical gradient → due to +ve luminal charge in late PCT
Descending loop of henle
% of K+ (Reabsorbed/Secreted)
–
Cellular Process
–
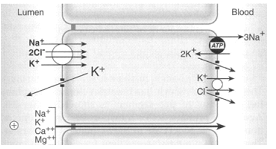
Thick Ascending Loop of Henle
% of K+ (Reabsorbed/Secreted)
30% reabsorption
Cellular Process
Reabsorption via active transport via paracellular route → +ve charged lumen generated by ion flux created by NKCCT transporter causes K+ to be reabsorbed by diffusion down its electrical gradient
DCT
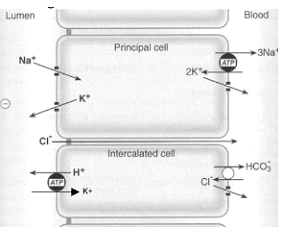
CCD – Principal Cell
% of K+ (Reabsorbed/Secreted)
Between 0% to > 15%
SECRETION
Cellular Process
2° active secretion K+→ via:
- Basolateral Na+/K+ATPase → (i) generates an electrochemical gradient that draws Na+ intracellularly from the tubular lumen (via the ENaC channel), and (ii) pumps K+ from peritubular capillaries into tubular cell
- The–vely charged lumen generated by influx of Na+across ENaCchannel → favours tubular secretion of K+
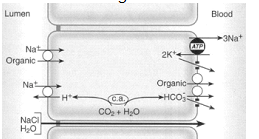
CCD – Type A Intercalated Cell
% of K+ (Reabsorbed/Secreted)
10% reabsorption
Cellular Process
H+ produced within tubular cell by hydration of CO2 using carbonic anhydrase H+ is then exchanged for tubular K+
MCD
% of K+ (Reabsorbed/Secreted)
5% reabsorption
Cellular Process
At the basolateral aspect:
K+ brought intracellularly by the basolateral Na+/K+ATPase is promptly recycled into the peritubular capillary via a basolateral K+channel and K+/Cl-co-transporter
Regulation
- Occurs MAINLY via control of K+ secretion at the distal nephron (CCD and LDCT)
- NOT via control of filtration or reabsorption
Circulating Factors:
(a) Plasma [K+]
- ↑ [K+] causes ↑ K+ secretion by → (i) Directly stimulating Na+/K+ ATPase in principal cells, and (ii) Directly stimulating Aldosterone release from adrenal cortex
(b) Aldosterone
- ↑ aldosterone causes ↑ K+ secretion by → ↑ production of Na+/K+ ATPase, K+ channels and ENaC Na+ channels in the principal cells
(c) Plasma pH
- Alkalosis via ↓ plasma [H+] causes ↑ K+ secretion by → stimulating Na+/K+ ATPase in principal cells
Luminal Factors:
(a) Flow of tubular fluid in DCT and CCD
- ↑ tubular fluid flow causes ↑ K+ secretion by → maintaining ↓ luminal [K+] (Ie. continuously washing it away) [also cuz increase flow means increase Na]→ permits passive diffusion of K+ ↓ its [ ] gradient into tubular lumen
(b) ↑ Na+ delivery rate to DCT and CCD → ↑ K+ secretion via ↑Na reabsorption via activity of Na/K ATPase
- (c) -ve lumen potential difference → ↑ K+ secretion
Author: Huiling Tan / Audrey Guo