65% Na+ & H2O reabsorbed @ PCT → ∴need to act here to score $$$
The osmotic force inhibits fluid reabsorption
Causes some Na+ loss
But the Na+ can be reabsorbed downstream @ thick asc. LoH
Natriuresis only 10% of filtered load (because acts so early)
In disease: glucose
Therapeutics: mannitol
Also
Impairs H2O reabsorption of Thin Desc. LoH because dissipates ISF osmotic gradient
↑RBF
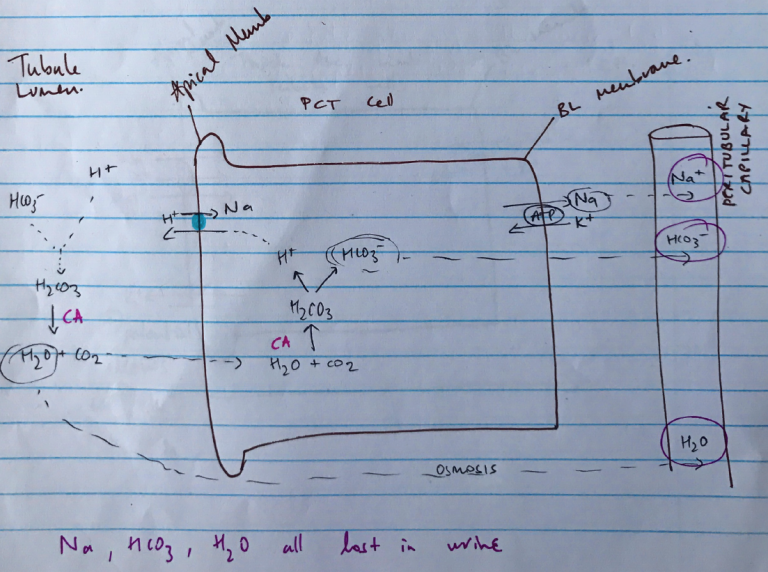
Carbonic Anhydrase Inhibitors
Enzyme CA present in PCT (heaps), Thick Asc. LoH & Intercalated cells of Collecting Duct
Present in tubule lumen & tubule cells
Drives equation: H+ + HCO3– ⮂ H2CO3 ⮂ H2O + CO2
Non-competitive inhibition of CA by acetazolamide blocks NaHCO3 reabsorption by:
↓H+ supply in tubule cell
H/Na antiporter can’t work
Na+ is not reabsorbed, H2O follows
1/3 Na+ reabsorbed by Na/H antiporter
Modest diuresis
NaHCO3 loss creates alkaline urine & metabolic acidosis in plasma
Loop Diuretics
Most efficacious diuretics
Inhibit Na/K/2Cl symporter on Thick Asc. LoH
↓Na & H2O reabsorption
25% Na+ reabsorbed at Thick Asc. LoH
& responsible for counter-current multiplication
∴kidney loses huge Na+ load & ability to concentrate urine
Occurs late in nephron ∴limited ability to reabsorbed Na+ later
Also
↑RBF
Loss of +ve potential from K+ recycling which aids Mg2+/Ca2+ reabsorption = Mg2+/Ca2+ loss
Thiazide Diuretics
Inhibits Na/Cl cotransporter on DCT → ↓Na+ reabsorption
DCT is impermeable to H2O
Acts in cortex, not medulla ∴no effect on counter-current multiplication
10% of filtered Na+ is lost
Also
↑Ca2+ reabsorption
By blocking Na/Cl transporter
↓IntraC Na+
∴↑activity of Ca2+/3Na+ exchanger
K+ Sparing Diuretics
Act at late DCT & collecting duct (because this is where K+ secretion occurs)
2 types:
SPIRO → antagonises aldosterone
AMILORIDE → blocks Na+ entry on Apical Na+ channel
Principle Cells
Spironolactone
Synthetic steroid
Competitive antagonist of aldosterone
Binds aldosterone receptor → inactivates
Prevents translocation of receptor & binding to DNA
∴
1) Failure to synthesise proteins which stimulate Na/K/ATPase pump
2) Upregulate apical Na+ channel
↓Na+ reabsorption & stops K/H+ secretion
Amiloride
Blocks apical Na+ channel
↓Na+ reabsorption & ∴Na/K/ATPase activity on BL membrane
Inhibition of K+ secretion is due to loss of voltage ∆
NB: Trimethoprim causes ↑K+ by same mechanism as amiloride!
Aquaretics
Antagonist V2 receptors on BL membrane
Inhibit action of ADH
Stops H2O reabsorption at collecting duct
Helpful to treat patient with hypo-osmotic ECF due to failure to excrete solute free H2O because ↑ADH from non-osmotic/non-haemodynamic mechanism (i.e. SIADH)