22A07: Exam Report
Write notes comparing the use of serum creatinine and creatinine clearance in the assessment of renal function in the critically ill
11% of candidates passed this question.
It was expected that candidates would define both components of the question, discuss the factors which affect serum creatinine and creatinine clearance and demonstrate their interrelationship.
More complete answers described the advantages, disadvantages and limitations of their use in critical illness. In many cases candidates failed to correctly define creatinine clearance.
Answers that scored well clearly utilised the above-mentioned breadth of knowledge and linked these to pertinent specific changes that may be associated with critical illness.
H4ii / 22A07: Write notes comparing the use of serum creatinine and creatinine clearance in the assessment of renal function in the critically ill
Creatinine
A small molecule produced by muscle metabolism. Eliminated by glomerular filtration and tubular secretion
Serum creatinine
A plasma concentration of creatinine
- Normally 60-100 umol/L (men > women)
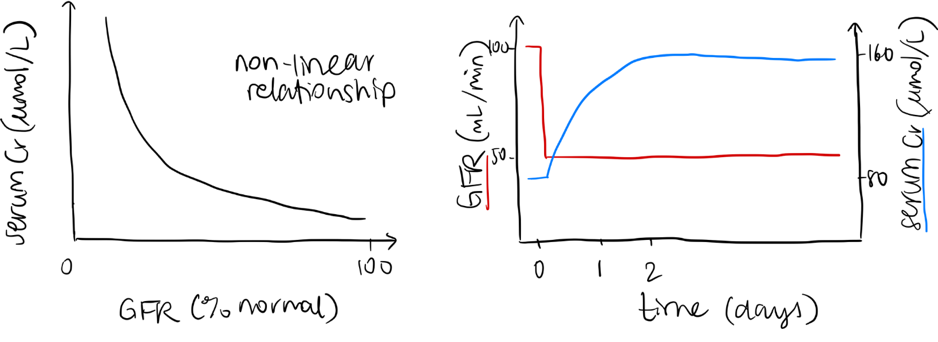
- Serum creatinine is inverse proportional to GFR at steady state
Creatinine clearance
The volume of plasma cleared of creatinine per unit time
Renal clearance = U x V / P
- U = urine concentration
- V = volume of urine produced per unit time
- P = plasma concentration
CrCl measurement:
- 24-hour urine collection and plasma level → Cl = UV/P
- Estimation using predictive equations
- Cockcroft Gault: estimates urine creatinine based on age, sex and body weight
- CrCl = (1.2x[140-Age] x Wt x Sex coefficient) / Cr
- Other formulas (MDRD, CKD-EPI) do not required weight and are better predictors of GFR
- Cockcroft Gault: estimates urine creatinine based on age, sex and body weight
Both used as surrogate markers of glomerular filtration rate
GFR
The rate of plasma filtered at glomeruli per unit time (125mL/min)
- Kidney is more complex than just filtration, so GFR itself is just a component of overall renal function
Factors affecting serum creatinine:
- Production of creatinine (can be highly variable)
- Muscle mass: age and sex affect
- Race
- Diet: ↑ with dietary protein intake, ↓ with fasting & vegetarian diet
- Muscle metabolism: BMR, temperature, activity
- Excretion of creatinine
- Creatinine is freely filtered at glomerulus and secreted by tubules
Serum Creatinine
Limitations
- Serum Cr is inversely proportional to GFR only when Cr production & glomerular filtration are at steady state – significant changes in GFR can occur before this is reflected in creatinine concentration
- Cr production can be highly variable
- g. in critically in patient may have cachexia, malnourishment, critical illness myopathy, muscular atrophy
- Large volume fluid resuscitation may dilute serum Cr, giving appearance of improved renal function
- Extracorporeal circuits can dilute or adsorb creatinine
- Dialysis clears creatinine → ↓serum Cr, but not associated with improvement in GFR
Advantages
- Readily available blood test
- Affordable
- Reproducible
Creatinine clearance
Limitations
- Actively secreted into tubules (to a small degree normally) so not truly reflective of GFR (overestimates)
- As GFR falls, proportion of Cr actively secreted by tubules increases → overestimates GFR when GFR is low
- Direct measurement cumbersome, takes ~24 hours so not rapidly available
- Estimation by calculation relies on incorporation of age, ethnicity, sex etc. for accuracy
- Estimation less reliable at extremes of weight, age, muscle mass and muscle metabolism → less suitable for use in critically ill patients
Advantages
- Endogenous substance, no exogenous administration required (compared to inulin)
- Measurement less affected by delay in Cr level with changes in GFR than serum Cr alone
Author: Emily Little