Ultrashort latency + ultrashort DoA → REMIFENTANYL
Ultrashort latency + short DoA → ALFENTANYL
Short latency, intermediate DoA → FENTANYL, PETHIDINE
Intermediate latency, long DoA → MORPHINE
Specificity & efficacy
Agonist
Partial agonist
Antagonist
Properties
CEUTIC all opioids are H2O soluble salt preparations
Physical Properties
Drugs
pKa
M
7.9
Pethidine
8.5
F
8.4
Alfentanyl
6.5
REMI
7.1
Methadone
9.3
Drugs
% unionised
M
23%
Pethidine
5%
F
10%
Alfentanyl
90%
REMI
67%
Methadone
1%
Drugs
n-octanol/H2O
M
1.4
Pethidine
39
F
860
Alfentanyl
130
REMI
17.9
Methadone
115
Drugs
VD CC (L/kg)
M
0.2
Pethidine
1.5
F
0.7
Alfentanyl
0.2
REMI
0.07
Methadone
–
Drugs
VD SS (L/kg)
M
3.2
Pethidine
9.4
F
4
Alfentanyl
0.86
REMI
0.4
Methadone
6
Drugs
PPB
M
35%
Pethidine
65%
F
85%
Alfentanyl
90%
REMI
80%
Methadone
85%
Drugs
Clearance
(mL/kg/min)
M
15
Pethidine
10
F
13
Alfentanyl
6.4
REMI
50
Methadone
1.5
Drugs
HER
M
0.7
Pethidine
0.8
F
0.9
Alfentanyl
0.4
REMI
N/A
Methadone
–
Drugs
Dist t ½ (min)
M
15
Pethidine
10
F
13
Alfentanyl
11.6
REMI
1 min
Methadone
0.9
Drugs
Elim t ½ (hrs)
M
3
Pethidine
3 – 5
F
3.6
Alfentanyl
1.6
REMI
5 min
Methadone
35
Drugs
t½ keo (min)
M
Pethidine
F
4 – 5mins
Alfentanyl
0.6 – 2.3
REMI
1.5 min
Methadone
Drugs
C5HT (after 4hr infusion)
M
Pethidine
F
4hrs
Alfentanyl
60 mins
REMI
4 min
Methadone
Ionisation = ↓lipid solubility
Low octanol/H2O coefficient = hydrophilic
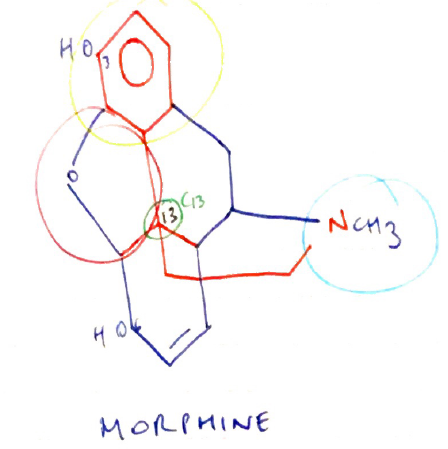
Morphine = poor lipid solubility → because -OH at C3 & C6
Structure
Amine group = essential for opioid agonist activity
+ve charge necessary to bind strongly to ANIONIC opioid receptor
Aromatic ring = phenol group attached to quaternary carbon
Quaternary carbon (C13) = carbon atom attached to four others → it is chiral & allows existence of enantiomers → attached to Phenolic Ring & Ethane Chain
Ethane chain ( – CH2 – CH2 – ) = separates quaternary carbons from N atom in amine group
Isomerism
Dextro & Levo enantiomers possible due to CHIRAL CARBON (C13)
Only levoratory exhibits agonist activity
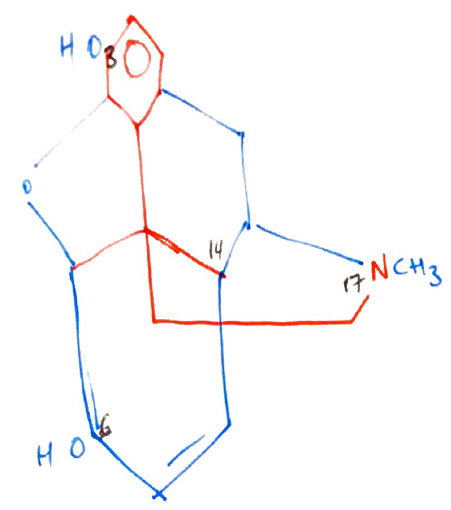
SAR
C3 = maximum opioid potency
Methylating this group (adding CH3) = makes codeine
Codeine x 10 less potent cf. M
But Codeine has reduced Metabolism → ∴ codeine has better OBA cf. M
C6 = addition of large side chains to C6 = ↑POTENCY because ↑lipid soluble e. HEROIN has a larger side chain at C6 (but this potency partially offset because also has masked the -OH at C3)
N17 = Substitution of phenylethyl group into nitrogen17 ↑agonist activity i.e. FENTANYL, as well as ↑lipid solubility
C14 = replacing nitrogen methyl group at N17 is coupled to C14 hydroxylation = formation of PURE ANTAGONIST → Naloxone
Indications, Administration, Dosing
Indications
Analgesia
Premed
Attenuate CV response to laryngoscopy
As a primary anaesthetic agent
Tx heroin withdrawal
Route
Enteral
Oral → M, Codeine, Endone, Tramadol, Methadone
PR → Oxycodone
Parenteral
SC, IM, IV → M, F, Pethidine
Neuraxial → M, F, Pethidine
Epidural = 10% IV dose
Intrathecal = 10% epidural dose
Topical
F, Buprenorphine
Dose → google ANZCA opioid dose equivalent for their PDF statement
Opioid
Morphine
Oral
30mg
Parenteral
10mg
Codeine
200mg
120mg
Endone
15mg
15mg
Pethidine
240mg
100mg
Fentanyl
–
100mcg
Alfentanil
–
1mg
Remifentanil
–
100mcg
Mechanism of Action
Opioids produce effect by binding µ opioid receptor
µ opioid receptor located throughout CNS, but concentrated in periaqueductal grey matter near 4th ventricle & substantia gelatinosa of dorsal horns of SC
Gi GPCR
Closure of voltage sensitive Ca2+ channels on presynaptic membrane → ↓intrac Ca2+
Post-synaptic stimulation of K-efflux → hyperpolarisation
Inhibition of AC → ↓cAMP
OVERALL → ↓cell membrane excitability, ↓transmission of nociceptive signals
Opioid Receptors
M receptor
2 subtypes
µ1 = supraspinal analgesia
Analgesia
Miosis
Euphoria
µ2 = spinal analgesia
Resp D
Inhibits GI motility
Euphoria
Dependence
Urinary retention
Pruritus
Prototype agonist = MORPHINE
δ-receptor
2 subtypes
Activation results in analgesia & resp depression
Spinal analgesia
Prototype agonist = ENKEPHALINS
k-receptor
3 subtypes
Activation results in:
Miosis
Dysphoria
Inhibition ADH release (diuresis)
Less analgesia
Dependence
Prototype against = DYNORPHINS
Opioid Receptor Activation
Endogenous peptide opioids (Endorphins, dynorphins, enkephalins) activate their specific opioid receptor
Overall ↓ neurotransmission
PRESYNAPTIC INHIBITION of NT release (Ach, DA, NA, sub P)
POST-SYNAPTIC INHIBITION of NT release
Opioid drugs mimic the actions of endogenous ligands
The effect the drug produces depends on:
Affinity for opioid receptor
+ve charged amine essential to bind anionic opioid R
↑opioid receptor occupancy = ↑opioid effects
Specificity of binding: µ, k, δ receptor
Efficacy of opioid
Full agonist = maximal biological response
Partial agonist = submaximal response
Antagonist = no biological effect
Mixed agonist-antagonist = simultaneously an agonist one receptor & an antagonist at another
Affinity & Efficacy of Opioids at Different Receptors
Full Agonist
Morphine
µ
+++
k
+
σ
Pethidine
+++
+
Fentanyl
+++
+
Alfentanil
+++
+
Remifentanil
+++
+
Partial Agonist
Buprenorphine
Partial Agonist
Nil
Tramadol
Partial Agonist
Nil
Antagonist
Naloxone
−−−
−
Pharmacodynamic Effects
CNS
Analgesia
Mainly due to peripheral opioid rec activation
↑pain threshold (↑stimulus required to activate nociception)
∆ pain perception/response → Europhia
Sedation
Dull C fibres > Sharp Aδ fibres
Sedation
Miosis
↑parasymp outflow of CNS
Resp
Ventilatory depression
↓CO2 responsiveness
Dose dependent respiratory depression
µ receptor of ventrally medulla agonism
↓brainstem response to CO2
Airway effects
Antitussive → by central opioid α agonism
Bronchospasm → histamine release provoked by opioids
↓ciliary activity
CVS
– VE INOTROPY
Pethidine causes marked myocardial depression
– VE CHRONOTROPY
Central vagal (X) excitation
Depression of AV Nodal Conduction (exception pethidine → tachycardia)
↓SVR
Histamine release → VD
GU
Urinary retention
Ureteric colic
Uterine contraction
∴ opioids cause SMOOTH MUSCLE CONTRACTION
NB: Opioids can worsen pain of ureteric colic ∴pethidine is preferred
GI
N&V → stimulation of µ receptors on CTZ floor 4th ventricle
↑smooth m. tone → delayed gastric emptying, reflux, constipation, biliary colic
Immunological
Histamine release (M > Pethidine > F)
NB: histamine release is not opioid R mediated & true allergy to opioids is uncommon
MSK
Pruritus → due to central effects & some histamine release
Usually post neuraxial administration
Intrathecal opioids cause pruritus by segmental excitation within SC