Xiii / PTX: Physiological consequences of a tension pneumothorax + Describe the anatomy relevant to insertion of intercostal catheter
Definition PTX: progressive build-up of air in the pleural space
Pathophysiology of Tension PTX
- Normally, in a spontaneously breathing patient, intrapleural pressure (P) is sub-atmospheric during resp cycle
- Due to opposing forces of chest wall & lung recoil
- PTX develops secondary to breach in visceral, parietal, or mediastinal pleura
- Defects create a 1-way valve
- Air enters pleural cavity on inspiration but cannot exit on expiration
- Consenquently, ↑intrapleural P results in:
- Ipsilateral lung collapse
- Chest wall expansion
- Diaphragmatic depression
- Mediastinal & contralateral compression
- Life threatening CV collapse due to impeding venous return (VR) & mediastinal compression
Mechanism of Effects
Lung
- ↓ lung vol, ↓VC, ↓FRC, ↓TLC, ↓RV → restrictive defect
- Expansion of pleural space
- Deflation of ipsilateral lung & expansion of chest wall
- ↓PαO2
- Lung collapse → creates areas w ↓V/Q
- ↑PA – α difference
- ↑ PVR
- Persistent hypoxaemia → hypoxic VC of pulmonary vessels
- ↑WoB
- Maximal resp efforts required to overcome the ↑ intrapleural P
Cardiovascular
- ↓CO
- ↑ intrapleural P → ↓VR → ↓preload & mechanical obstruction due to ↑intrapleural P → ↓CO
- ↑HR
- ↑sympathetic activity 2° to baroreceptor activation from ↓BP
- Compensatory due to ↓CO
Anatomy for ICC Insertion
- ICC: tube inserted into pleural space to allow drainage of contents
- Location → “Safe triangle”
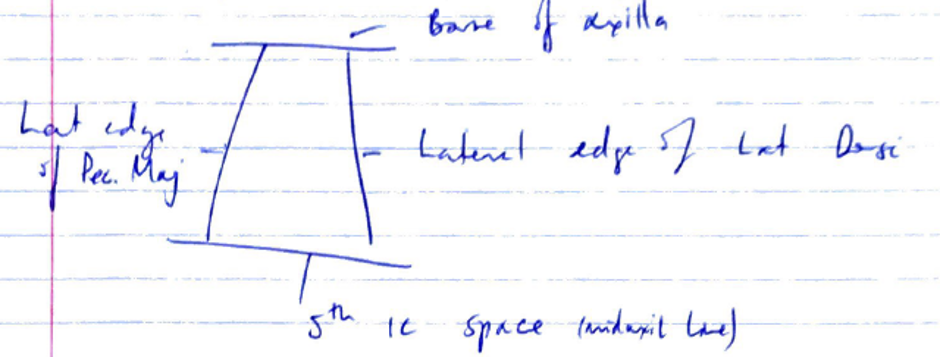
- Incision into 4th/5th IC space
- Layers from skin to pleura:
- Skin
- Fascia
- External IC m.
- Internal IC m.
- Innermost IC m.
- Parietal fascia of thorax
- Parietal pleura
- Muscle of IC space innervated by neurovascular bundle → sits in groove of rib above
- VAN from sup. → inf.
- Bundle lies b/w innermost and internal IC m.