19B16: Exam Report
Compare the structure, function and coronary circulation of the right and left ventricles.
27% of candidates passed this question.
The question sought information on the structure (anatomy), function (physiology) and vascular supply of the right and left ventricle. Good answers provided detail in each section e.g. values for ventricular pressure rather than simply stating “high- and low-pressure systems”.
Many marks may be gained by a simple anatomical description & labelled PV loop for each ventricle. Many candidates focussed solely on the coronary circulation, to which only a proportion of the marks were allocated.
G1ii / 19B16: Compare the structure, function and coronary circulation of the right and left ventricles
Tips
- Suggest a table with all the headings from the question and ensure similar amounts of information in each
- Include broad concepts and some specific numbers
- Graphs can prevent use of too many words if able to do quickly
- This answer has more information than can be written in 10mins – include ~50-80% of each section and should easily get a pass mark if sufficient detail
- Can also include more detail in sections where you know it!
Structure
Left Ventricle
Right ventricle
Left Ventricle
Inflow: LA → mitral valve
- 2 cusps (anterior and posterior)
- Papillary muscles connecting trabeculae to cusps via cordae tendinae
Right ventricle
Inflow: RA → tricuspid valve
- 3 cusps (medial, anterior, inferior)
- Papillary muscles connecting trabeculae to cusps
Left Ventricle
Ventricle:
- Thicker LV muscle wall x3 compared to RV
- Significant trabeculation
- More conical shape of cavity – thinner towards apex
- Dimensions: 25-40mm base, 15-25mm distal
- Smooth outflow tract supports AV, anterior to MV
Right ventricle
Ventricle:
- Thinner RV muscle wall
- Inflow tract supports TV, trabecular
- Muscular infundibuloventricular crest separates inflow and outflow tracts
- Dimensions: 20-35mm systole, 40-50mm diastole
- Outflow tract – smooth, directed up and right towards pulmonary trunk
Left Ventricle
Outflow: aortic valve → Aorta
- 3 cusps (right posterior, left posterior, anterior)
- Aortic sinuses above give rise to coronary arteries
- Left posterior → left main coronary
- Anterior → right coronary
Right ventricle
Outflow: pulmonary valve → pulmonary trunk
- 3 cusps (posterior, right
Function
Left Ventricle
Right ventricle
Left Ventricle
Delivers oxygenated blood to the systemic circulation for tissue perfusion
- High resistance
- High pressure
Normal pressures:
- LVSP 100-140mmHg
- LVDP 3-12 mmHg
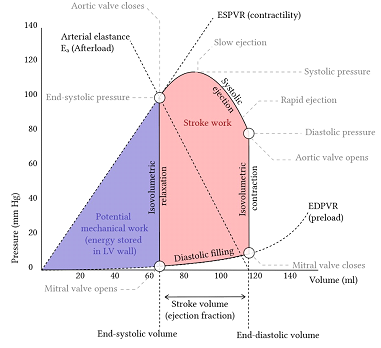
LV pressure-volume loop
Right ventricle
Delivers deoxygenated blood to the pulmonary circulation for oxygenation
- Low resistance
- Low pressure
Normal pressures:
- RSVP 15-25mmHg
- RVDP 0-8mmHg
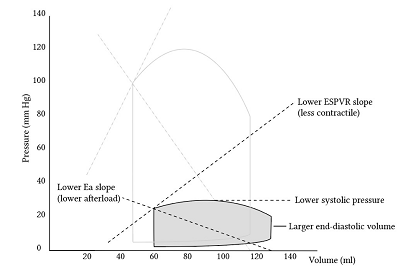
RV pressure-volume loop
Coronary Circulation
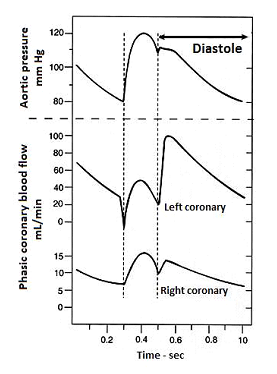
This section is less necessary – pick out key elements. Graph is only useful if able to draw quickly but if you’ve already said that flow is diastolic vs whole cardiac cycle and talked about different pressures it does not add extra information
O2 demand depends on:
- Myocardial wall stress = transmural pressure x radius / 2x wall thickness
- HR – affects both ventricles similarly
- Contractility
- (+ BMR, external work, electrical activation)
Supply depends on
- Coronary flow – from 5% of CO (250ml/min), up to 4x increase with high demand
- O2 content – normally fairly constant ~ 20.4ml/dl
- O2 extraction – near constant ~ 70%
Left Ventricle
Right ventricle
Left Ventricle
Anatomy:
- LM → LAD and LCx
- LAD → anterior wall, anterior 2/3 of septum
- LCx → inferolateral wall
- PDA made up of dominant RCA or LCx → posterior wall and 1/3 of septum
Right ventricle
Anatomy:
- RCA → most of RV wall
- PDA made up of dominant RCA or LCx → posterior wall and 1/3 of septum
- LAD → anterior 2/3 of septum
Left Ventricle
Higher O2 demand due to
- High transmural pressure
- Larger radius
- Slight offset by thicker walls
- Higher muscle mass – contractility
Right ventricle
Lower O2 demand due to
- Low transmural pressure
- Smaller radius
- Smaller muscle mass – contractility
Left Ventricle
Supply:
- CBF = diastolic P(aorta) – LVDP or RAP / CVR
- (whichever is higher of LVDP or RAP ie coronary sinus pressure)
- Flow occurs in diastole only
- Decreased diastolic time → decreased perfusion with increased HR (+ higher demand!) → ischaemia risk
Right ventricle
Supply:
- CBF = MAP – mRVP / CVR
- Flow throughout cardiac
Author: Manon Audigé