2 major causes of arrhythmias are:
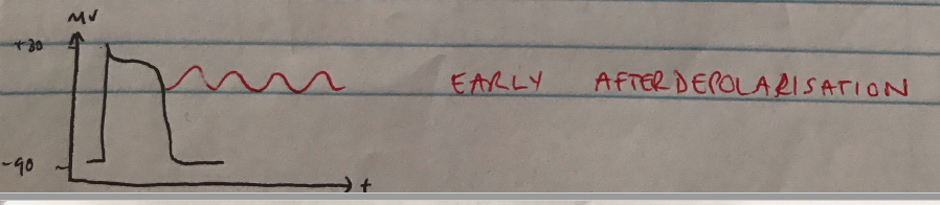
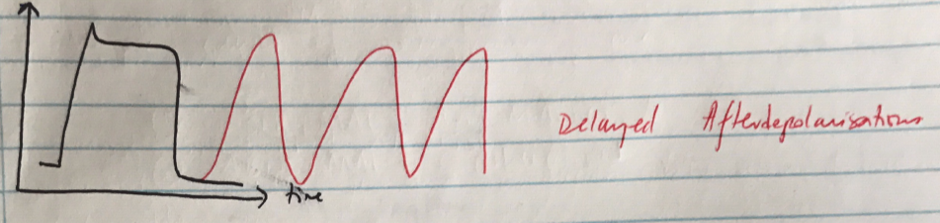
Fast AP cells can undergo spontaneous depolarisation in Ph 3-4 (relative refractory period)