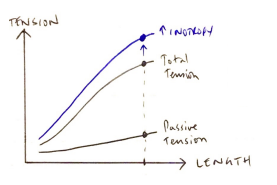
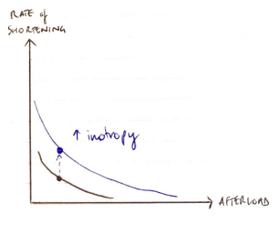
Contractility = the intrinsic ability of myocardial fibres to shorten, independent of preL & afterL
(it augments force of myocyte contraction via SLIDING FILAMENT)
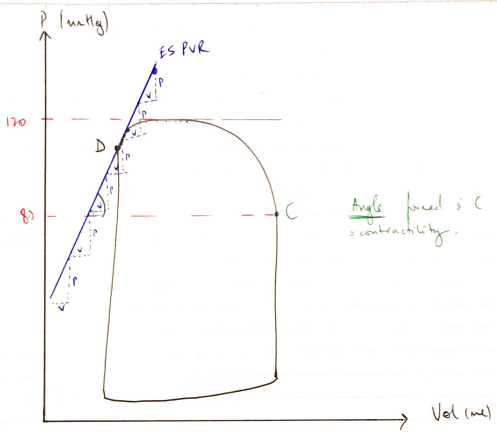
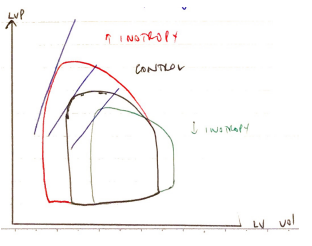
P/V = Elastance
∴slope of this line is elastance, which is KA E0 → where the PV loop falls on the ESPVR line