Describe the forces that result in fluid exchange across capillary membranes.
57% of candidates passed this question.
The expected answer included a clear explanation of Starling’s forces, including an understanding of the importance of the relative difference along the length of the capillary, with approximate values and examples of factors that influence them. Some explanation of what contributed to the hydrostatic or osmotic pressure gained more marks than merely stating there was a pressure. Several candidates digressed to Fick’s law of diffusion or intracellular flow of ions which was not directly relevant to capillary flow.
16B19: Exam Report
Describe how Starling forces determine fluid flux within the pulmonary capillary bed.
25% of candidates passed this question.
The equations for nett fluid flux and for nett filtration pressure were incorrect in many answers.
Better answers presented the equations and discussed each of the elements as relevant to the pulmonary capillary bed, including difference from systemic capillary beds.
Mention of the role of lymphatics and of the effect of surfactant, left atrial pressure, gravity and posture gained marks, also.
G4i / 18B16 / 16B19: Describe how Starling forces determine fluid flux within the pulmonary capillary bed Describe the forces that result in fluid exchange across capillary membranes
Capillary wall is a SEMI-PERMEABLE MEMBRANE
Permeable to H2O, solutes
Impermeable to large proteins
Produces a plasma ultrafiltrate
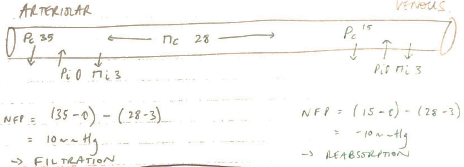
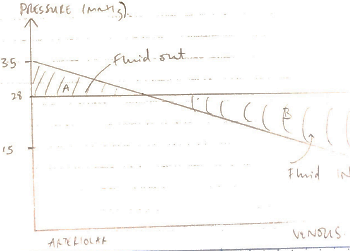
Filtered by BULK FLOW through capillary wall by opposing hydrostatic + oncotic pressures
The function of this bulk flow is the distribute fluid between intravascular & extravascular compartments → no nutritional benefit
Starling Forces
Hydrostatic & oncotic pressures described by ∆ Starling Forces: