G6i: Describe the ECG changes seen with hyperkalaemia (30 marks) + Outline the pharmacological principles of drugs used in the management of severe hyperkalaemia (70 marks)
Definition ↑K+ = K > 5.5mol/L
Role of K+
Major intracellular cation → maintains intracellular tonicity
Generation of RMP
Na/K/ATPase
Problem of ↑K+
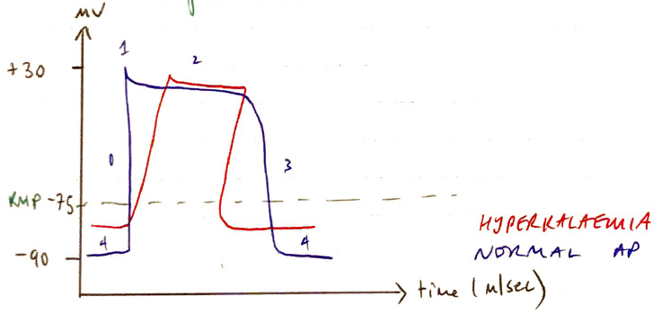
RMP is less negative ∴ membrane more excitable
Refractory period initially ↓ but as K > 8mol/L, induces post-repolarisation refraction which prolongs refractory period
Shortened AP duration
↓conduction velocity
VMAX = rate of rise of AP
VMAX ∝ RMP because the membrane potential at onset of depol. determines the no. of Fast Na+ channels activated
As RMP becomes less negative = less Na+ channels activated → ↓VMAX
↓VMAX = slows impulse conduction through myocardium
ECG ∆ of ↑K+
K+ (mol/L)
K+ (mol/L)
Reason
5.5 – 6.0
Peaked Tw
Shortened repolarisation
Shortened duration AP
↑myocyte excitability
> 6.5
P waves fluttering
Slowed conduction velocity
> 7.0
Widened QRS
Prolonged PR
Slowed conduction velocity further as ↑RMP
> 8.5
QRS widens further to blend with T-wave → SINE WAVE
Hyperkalaemia MX
Principles of Tx
Stabilise myocardium
More K+ intracellularly
Excrete K+ from body
Tx cause
1) Stabilise myocardium
Drug: Ca2+ gluconate 10%
Dose: 10mL
Onset: 3 mins
Duration: 30 – 60 mins
MoA: 3 mechanisms
Threshold: Ca2+ shifts threshold to be less -ve so difference is maintained
VMAX: restoring threshold will normalise VMAX & Na+ channel activation to restore conduction velocity
Impulse propagation: Ca2+ dependent AP propagation (SA & AV nodes) restored