PAC = the PAC is a balloon-tipped thermodilution catheter 110cm long, that is inserted via a large vein & floated into the PA
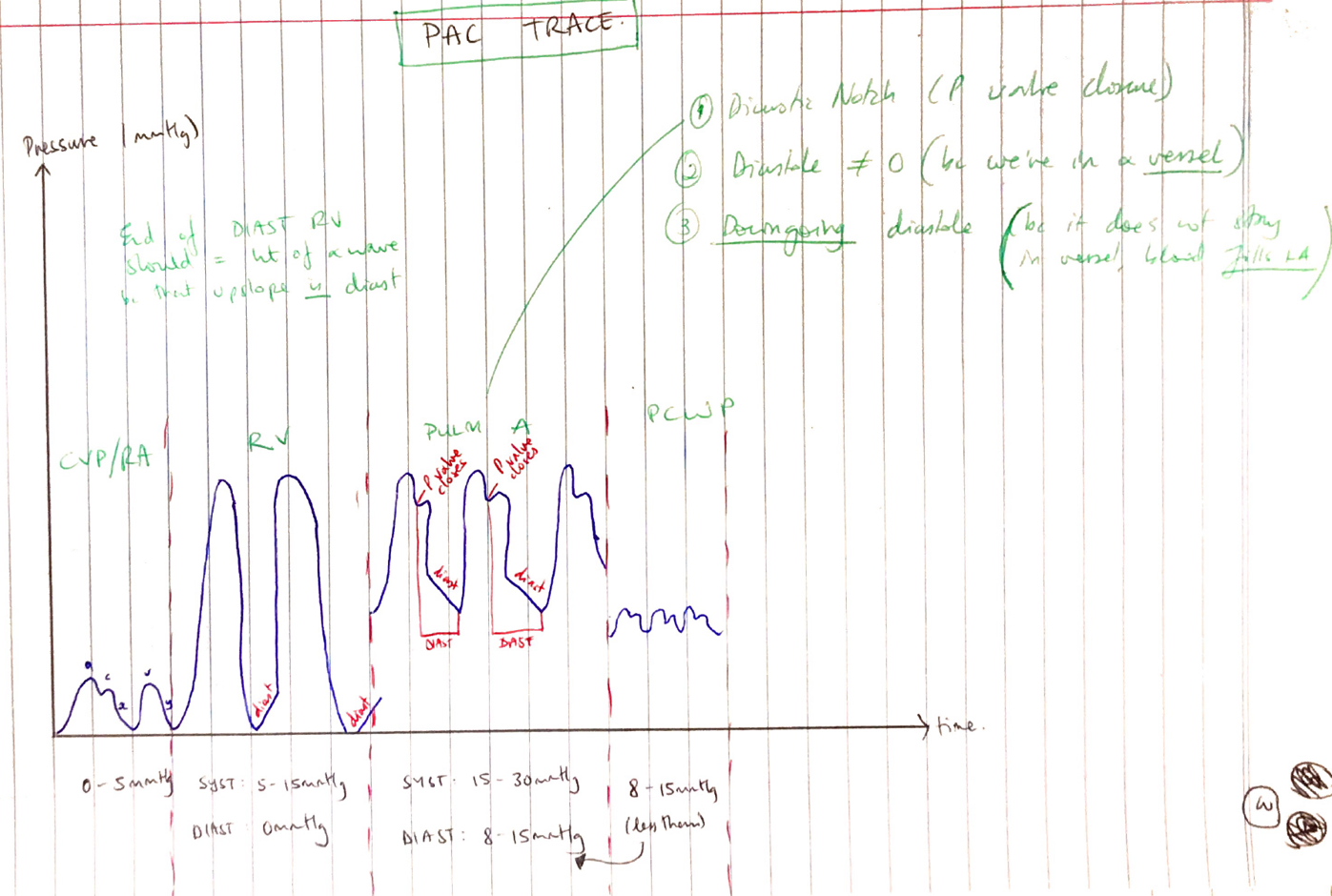
RA pressure
RV pressure
PA pressure
PCWP
CO
Mixed venous oxygen saturation
HR
CI
SV
SVI
SVR
SVRI
PVR
PVRI
CaO2 – arterial oxygen content
CvO2 – mixed venous oxygen content
DO2 – oxygen delivery
VO2 – oxygen consumption
Slow bolus
Inaccurate vol.
Inaccurate temp.
Malpositioned
Thermistor wedge
Resp fluctuations (should be measured at expiration)
TR
HCT
Arrhythmias