Most questions lacked a systematic approach to the question and specific detail. The relationship between systemic toxicity (CNS and CVS) and plasma levels should be described. Many candidates did not clearly state that CNS toxicity occurs at lower plasma levels that CVS toxicity. Factors that affect toxicity (e.g. drug factors, patient factors, interactions) needed to be elaborated with some detail. Patient factors such as age, pregnancy, acidosis, hyperkalaemia, hepatic failure were often omitted. Finally, marks were also awarded for noting methaemoglobinaemia as possible toxicity and the existence of specific therapy (intralipid).
K2ii / 18B19: Describe toxicity of local anaesthetic agents
Definitions
Toxicity = occurs when the physiological response to a drug is an adverse effect
Classification of LA Toxicity
Systemic Toxicity
Local Neurotoxicity
Hypersensitivity Reactions
Agent Specific Toxicity
a. MetHb w Prilocaine
b. Cocaine toxicity
Systemic Toxicity
Excess plasma concentration of a drug due to absorption and distribution of drug distant to its entry point
The most common adverse reaction to LAs is systemic toxicity
Usually due to accidental IV injection / overdosage
PPB sites become quickly saturated and unbound drug is available to diffuse into CNS & conducting tissue of heart
Symptoms of LA toxicity correlate well with plasma levels:
\( \textbf{CC/CNS Ratio = } \frac{\text{Blood level for cardiovascular}}{\text{Blood level for convulsions}} \)
CC/CNS Ratio = the ratio of blood levels required to produce irreversible cardiovascular collapse cf the blood levels required to produce convulsions
CC/CNS Lignocaine = 7
CC/CNS Bupi = 2.7
Therefore, x7 much as much drug will induce irreversible CVS collapse cf the dose required to produce convulsions, thereby providing enough warning of toxicity before CVS collapse
Mechanism of Toxicity
LAs are Na ch inhibitors, therefore have high activity at CNS & CVS
Non-iniosed drug crosses myelin sheath & axonal membrance
Dissociates into ionised form (intracellular pH is lower)
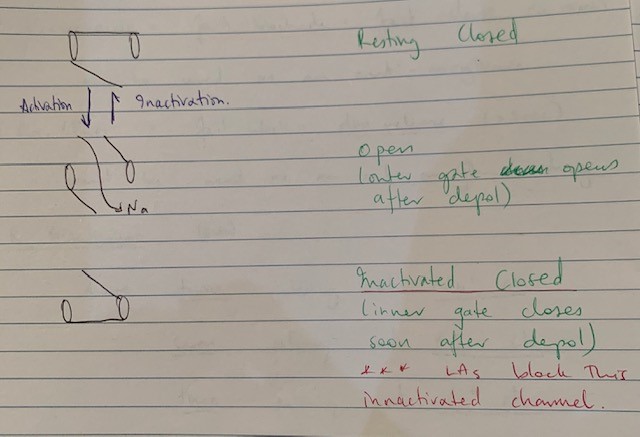
Ionised form binds to activated Na ch & produces a blockade in the inactivated state
CNS Toxicity
2 stage process:
Blocking Na ch of inhibitory neurons = unopposed excitation = convuslsions
Total neuronal blockade = CNS depression
Slowing/silent EEG
Coma
CVS collapse
CVS Toxicity
Direct
Negative inotropy
Delayed conduction
Indirect
Autonomic outflow block
CVS centre of midbrain depression
Results in HTN & tachycardia secondary to CNS excitation
Then myocardial depression and ↓CO → peripheral VD & severe ↓BP → brady/dysrhythmia → Cardiovascular collapse
Factors which Increase the Risk of Toxicity
Ceutic
R enantiomer;
Racemic (Bupi) mixtures
Twice as potent at Na channels
Seven times as potent at K channels
Three times as potent at Ca channels
PK
A
Diffusion from site of injection obeys Fick’s Law:
\( \textbf{Rate of Diffusion = } \frac{\text{SA}}{\text{T}} \textbf{ x } \frac{\text{Solubility}}{\sqrt{\text{MW}}} \textbf{ x } (C_2 – C_1) \)
Dose: ↑dose = ↑ rate of diffusion
Max doses:
Drug
Maximum Dose
Adrenaline – can be added to LAs for its potent VC properties ↓rate of absorption and therefore ↓rate of rise of plasma levels. But, it carries its own risk of arrythmias & tachycardia
Drug
Cocaine
Maximum Dose
1.5-2.0mg/kg (independent of adrenaline) to maximum of 100mg
Drug
Prilocaine
Maximum Dose
8mg/kg (plain) to maximum of 400mg
10mg/kg (+Adr) to maximum 600mg
Drug
Lignocaine
Maximum Dose
3-5mg/kg (plain) to maximum dose of 200mg
7mg/kg (+ adrenaline) to maximum of 500mg
Drug
Bupivacaine
Maximum Dose
2mg/kg (independent of adrenaline) to maximum of 150mg
Drug
Ropivacaine
Maximum Dose
<3mg/kg (independent of Adr) to maximum 200mg
Injection site: ↑degree of vascularity = ↑plasma concentration; IC > Epidural > subcutaneous