15B16: Exam Report
Describe ammonia metabolism and excretion (70% of marks). Outline the pharmacology of lactulose (30% of marks).
37.5% of candidates passed this question.
It was expected candidates would identify sources of ammonia (colon from metabolism of proteins, kidney, small amounts from breakdown of red blood cells and metabolism in muscles). The liver converts all circulating ammonia to urea (the urea cycle) (2NH3+CO2 = urea +H2O).
Urea then undergoes enterohepatic circulation (25%) or is excreted by kidneys (75%). Ammonia (NH3) is lipid soluble and diffuses into the interstitial cell and tubular fluid by non-ionic diffusion where is buffers H+ to become non diffusible NH4+. No candidate mentioned enterohepatic circulation and most answers had very little detail on the metabolism and excretion and lacked depth.
Lactulose is a non absorbable synthetic, non-digestible disaccharide. It is an osmotic laxative fermented by gut flora producing metabolites (such as acetate) which have osmotic and peristalsis-stimulating effects, and methane causing in flatulence.
Few could describe how lactulose decrease absorption of ammonia and a surprising number of people did not even state that lactulose was an osmotic laxative.
O2i / 15B16: Describe ammonia metabolism & excretion (70 marks). Outline the pharmacology of lactulose (30 marks)
Definition
Ammonia = major metabolic by-product of protein and nucleic acid catabolism
Present in equilibrium body fluid as NH3 and NH4+:
NH3 + H+ ⇔ NH4
- pKa 9.25 therefore at physiological pH, there is excess of ionised form
- NH3 diffuses freely
- NH4 is carried to the liver by active transport
- Blood Ammonia < 35mmol/L
Ammonia Source
- Most ammonia is formed in extrahepatic tissues (kidney, intestine)
- Most ammonia is transported to liver as a-acids
- XS a-acids are degraded by transamination, deamination and decarboxylation
Ammonia Transport to Liver
2 mechanisms

b) Pyruvate → Alanine → Liver
Ammonia Detoxification by Liver
90% of nitrogen enters urea cycle
2NH4+ + CO2⇔Urea + 2H+ + H2O
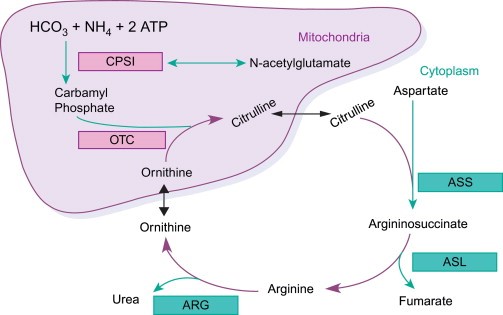
- Formation of CARBAMOYL PHOSPHATE from Ammonia & HCO3
- Condensation of carbamoyl phosphate with ORNITHINE → CITRULLINE
- Citrulline condenses with ASPARTATE → ARGININOSUCCINATE
- Arginosuccinate is hydrolysed to FUMARATE + ARGININE
- ARGININE is cleaved → UREA + ORNITHINE
- ORNITHINE re-enters mitochondria and combines with CARBAMOYL PHOSPHATE to form CITRULLINE
- UREA ⇔25% Enterohepatic Circulation, 75% excreted by kidneys
The Urea Cycle removes ammonia and irreversibly removes HCO3–
But the whole process is acid-base neutral as the HCO3– made is removed almost as soon as it’s made:
2 a-acids → 2NH4+ + 2HCO3– → Urea/Glutamine
Enterohepatic Circulation
- Urea diffuses → blood → intestine
- Bacterial Urase cleaves Urea to liberate NH3 + CO2
- Some NH3 → feces
- Some NH3 → reabsorbed into blood → via Enterohepatic Circulation
- Neomycin ↓bacterial degredation of Urea in intestine
Ammonia/Urea Handling by Kidney
- Urea constitutes half of solute load in urine
- Urea freely filtered by glomerulus
- Half is reabsorbed in PCT
- An amount equal to reabsorbed portion is secreted back into LoH
- Half is reabsorbed again in Collecting Duct
- Overall half filtered load is excreted
Ammoniagenesis From Glutamine
- Glutamine from liver
- Taken up by PCT cells
- In PCT: Glutamine → NH4+ + HCO3–
- This new HCO3– diffuses into interstitium
- NH4+ is secreted into tubule lumen via transport exchanger for Na+
- Eventually it is excreted in urine
Lactulose
Chemical
Non-absorbable synthetic, non digestible dissacharide
OSMOTIC LAXITIVE
Presentation
Tablets, syrup
Dose
30ml bd → qid for Hepatic Encephalopathy
Route
Oral
MoA
A synthetic sugar of Fructose & Galactose
In colon broken down by colonic bacteria to monosaccharides
This ↑osmotic pressure = ↑water retention in stool
Also draws NH3 out of body (same way it draws out H20)
PD
GI: ↑ water retention of stool
PK
A
Not absorbed/no human enzyme can hydrolyse
D
N/A
M
Metabolised by gut bacteria
Metabolites have osmotic & peristaltic effect
Metabolised completely (no lactulose in faeces)
E
Fecal
T1/2 = 2hrs
Adverse Effects
Diarrhoea
Bloating
Gas