G3iv / 16B07: Compare and Contrast the supply and demand of O2 for the RV and LV
16B07: Exam Report
Compare and contrast the supply and demand of oxygen for the right and left ventricle.
29% of candidates passed this question.
An integrated answer to supply and demand of oxygen was expected, as a comparison between the right and left ventricles. Many candidates concentrated on differences not similarities. Myocardial oxygen demand was in general poorly described.
About 85 – 90% of oxygen demand is for internal work (major determinants wall tension 30 – 40%, heart rate 15 – 25%, myocardial contractility 10 – 15%, basal metabolism 25%). 10 – 15% of oxygen demand for external work or pressure volume work, determined by MPAP x CO.
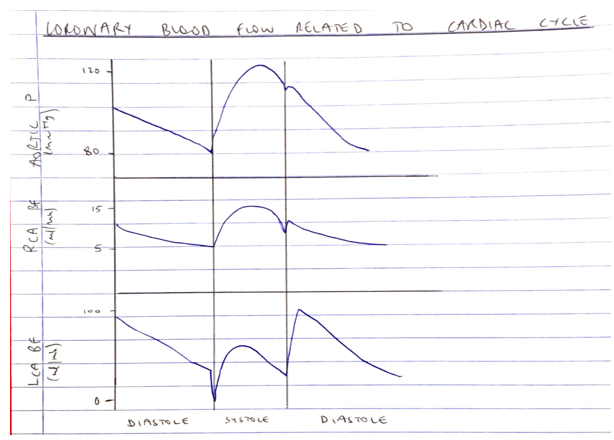
It was expected answers would comment on the phasic nature of coronary blood flow which differs between left and right and the consequence of this to subendocardial oxygen supply during systole usually. Coronary blood flow is affected by coronary perfusion pressure (determined by aortic pressure and RV pressure) & coronary vascular resistance (determined by autoregulation, metabolic factors, humoral factors, nervous control interacting with local endothelial factors)
Generally, coronary blood flow is tightly coupled to oxygen demand/consumption due to high basal oxygen consumption (8 – 10 ml/ min/100g) and high oxygen extraction ratio (75%). Better answers noted that oxygen supply can only be increased to cope with increased demand only by increased coronary blood flow.
G3iv / 16B07: Compare and Contrast the supply and demand of O2 for the RV and LV
Define
Heart = aerobic organ → CANNOT TOLERATE O2 DEBT
- Will use any substrate available
- Glucose, lactate, ketones, FA
- 40% glucose, 60% other
- Insulin glucose uptake by myocytes
Quantify
Blood flow = 250ml/min
5% CO
O2 consumption 30ml/min
10% of O2 consumption
High extraction ratio = 80%
If demands increase it cannot extract any higher, it is FLOW LIMITED
Classify
Coronary Blood Supply
Coronary Anatomy
Right Ventricle
R cusp of AoV
Gives off
- Conus Branch
- SA branch
- AV nodal branch
- R Marginal
- Post descending A (dominance
Left Ventricle
L cusp of AoV
- LCx
- LAD
Right Ventricle
Left Ventricle
Coronary
Blood Flow
CBF = CPP/CVR
CPP = Aortic P – (larger of) Ventricular P or RAP
Coronary
Perfusion Pressure
Right Ventricle
Throughout systole & diastole
Driven by Aortic pressures
RV SYST CPP
= Aortic Syst P – RVP
= 120 – 25
= 95mmHg
RV DIAST CPP
= Aortic Diast P – RAP
= 80 – 5
= 75mmHg
Left Ventricle
Early systole → compression → CBF briefly reverses
Mid-late systole → follows aortic P
Diastole → maximal BP as compression lifted, then falls as aortic P falls
LV SYST CPP
= Aortic Syst P – LVP
= 120-120
= 0mmHg
LV DIAST CPP
= Aortic Diast P – RAP
= 80-5
= 75mmHg
Right Ventricle
Left Ventricle
Coronary
Vascular
Resistance
R = 8hL/pr4
Radius is biggest influence
Determined by:
- Metabolic
- Pathology
- Autoregulation
- ANS
- Humoral
- Drugs
Ventricular Demand
Myocardial O2 consumption determined by:
Wall Tension (40%)
Basal Metabolic Activity (25%)
HR (25%)
Contractility (15%)
External work (10-15%)
Electrical Depolarisation (1%)
Right Ventricle
Left Ventricle
Wall Tension
AfterL gives rise to Wall Tension in the ventricle ∴can be thought of as wall tension required to overcome impedence to eject blood into ventricle WALL TENSION Wall T = (Transmural P x Radius) / (2 x Thickness) Transmural P Radius Thickness – Thickness of LV greater due to higher afterload it works against OUTFLOW TRACT RV pumps blood against a low resistance circuit (PVR) and therefore in health should not require as much as the LV SVR is primary determinant of LV afterL LV has to pump against a much higher afterload and thus has much more demand |
Right Ventricle
Left Ventricle
Basal Metabolic Activity
Basal Metabolic activity = basal O2 consumption = 8ml/100g/min both ventricles
Right Ventricle
Left Ventricle
Heart Rate
Majority of CBF occurs in diastole;
In LV blood supply occurs only in diastole, so tachycardia reduces diastolic filling time and greatly compromises the actual supply → Subendocardium most susceptible, no flow during systole
Tachycardia will also increase the energy requirements of myofibrils from lengthening and shortening and increase demand for substrate and O2
Right Ventricle
Left Ventricle
Contractility
Intrinsic ability of myocardial fibres to shorten, independent of preL & afterL
LV will have more demand than LV owing to larger m mass
Right Ventricle
Left Ventricle
External work
Does not correlate well w O2 consumption
Refers to volume work, both ventricles eject similar volume so this work is similar
Right Ventricle
Left Ventricle
Electrical depolarisation
Similar level of contribution
Measuring Myocardial O2 Consumption
- Requires measuring arterial + venous O2 content & application of FICK PRINCIPLE
- Unrealistic to achieve
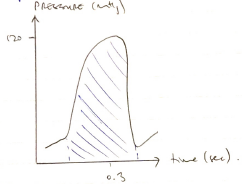
- When myocardial CONTRACTILITY is steady, measuring TENSION TIME INDEX will reflect myocardial O2 consumption
- Author: Krisoula Zahariou