Classify anti-arrhythmic drugs by mechanism of action, giving examples of each (75% of marks). Describe the electrophysiological and ECG effects of sotalol (25% of marks).
88% of candidates passed this question.
Most answers displayed a good knowledge of the Vaughan Williams classification, classes I to IV and the relevant electrophysiological characteristics of the classes.
Answers should also have included mention of other antiarrhythmics, such as digoxin, magnesium and adenosine. The second part of the question required comment about K ion blockade and its effects. It was helpful to mention prolongation of QT and risk of torsade. Most answers omitted reference to its being a racemic mixture, with different actions of the isomers.
G7iii / 16B21: Compare and contrast the mechanism of action, pharmacokinetics and adverse effects of digoxin and sotalol
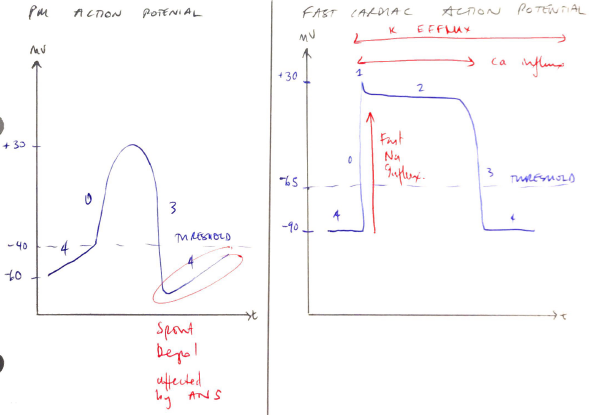
Arrhythmia = abnormal rate, generation, propagation of an AP
Caused by:
Abnormal PM activity
Abnormal impulse propagation
∴ Antiarrhythmic:
↓ectopic PM activity
Modify conduction
By altering:
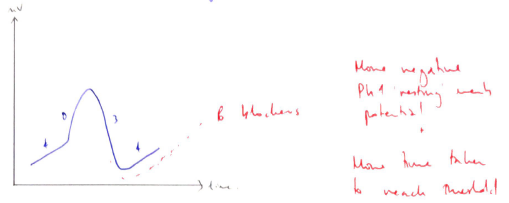
Slope Ph 4: β-blockers, adenosine, ↑vagal tone
Threshold AP: Na+ channel blockers, CCB
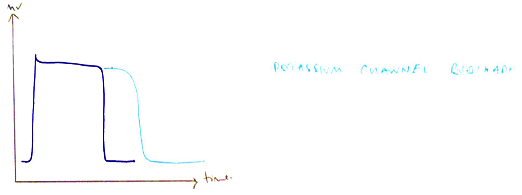
AP duration: Na+ channel blockers, K+ channel blockers
Maximum diastolic potential: adenosine by hyperpolarisation
V – W classify antiarrhythmic in groups based on electrophysiological characteristics → based on micro-electrode studies
Class
I
SODIUM CHANNEL BLOCKERS
Example
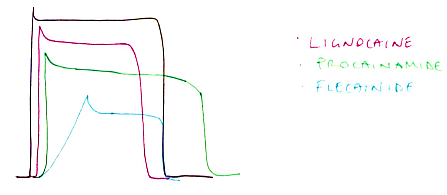
IA – PROCAINAMIDE
IB – LIGNOCAINE
IC – FLECAINIDE
Mechanism of Action
Moderate Na+ channel block, ↑refractory period
Weak Na+ channel block, shortens AP
Strong Na+ channel block, no effect refractory period
Class
II
β-BLOCKERS
Non-selective
Selective
Intrinsic sympathomimetic activity
Example
PROPANOLOL
METOPROLOL
LABETALOL
Mechanism of Action
Antagonises effects of catecholamines at β receptors
In heart: – CHRONO, – DROMO, -INOTROPY
↓slope Ph 4 = more time to reach threshold = ↓discharge rate