Define respiratory compliance, include its components and their normal values (25% marks). Explain the factors that affect respiratory compliance (75% marks)
27% of candidates passed this question.
This question covers a core principle of respiratory physiology and would be expected to have a high pass rate. Most candidates were able to provide a concise definition and distinguish between the different types of compliance.
The imprecise use of terminology often created the impression of a lack of fundamental understanding of this key concept.
Candidates are encouraged to be accurate and concise in their definitions.
A lack of detail in describing the relevant components of compliance and the factors that influence it, immediately limited the capacity of some candidates to achieve an adequate score.
Most candidates provided less than half of these factors and only provided a list rather than explaining how compliance was impacted.
Marks were maximised by dividing the impacts into those that altered lung compliance versus those that impacted on chest wall compliance, and the better candidates explained how and why compliance was affected. Confusion often arose from the imprecise use of arrows with the result that candidates frequently demonstrated an incorrect fact in relation to the direction of the arrow.
Candidates are reminded to take care when using abbreviations or arrows to ensure they are not relying on the examiner to interpret a cause and effect relationship.
19B17: Exam Report
Explain respiratory compliance and outline the factors that affect it.
51% of candidates passed this question.
Answers were generally well structured.
Better answers described lung and chest wall compliance and the pressures which are used to calculate compliance.
Better answers displayed an understanding of dynamic, static and specific compliance and provided a reasonably comprehensive list of the physiological factors affecting chest and lung compliance.
17A14: Exam Report
Define respiratory compliance (20% of marks). Describe the factors that affect it (80% of marks).
54% of candidates passed this question.
This question was generally well answered with good structure.
14A15: Exam Report
What is lung compliance and how is it measured?
34% of candidates passed this question.
There was a good understanding of the definitions of compliance but many candidates failed to clearly demonstrate an understanding of the difference between static and dynamic compliance.
Many candidates had little knowledge of how compliance is measured. It was expected that descriptions of methods to measure static and dynamic compliance would be provided.
There were frequent errors in descriptions that were provided.
F3ii / 22A03 / 19B17 / 17A14 / 14A15: Define compliance (static, dynamic, specific), its measurement, and relate this to the elastic properties of the respiratory system
Definition
Compliance = measure of distensibility of matter
Respiratory System Compliance is made up of
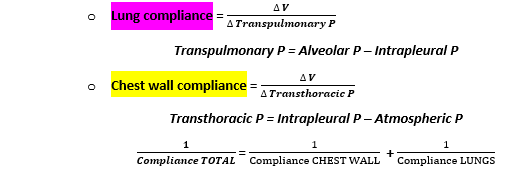
Lung Compliance = 200ml/cmH20
CW Compliance = 200ml/cmH20
They are in parallel ∴Total compliance = 100mL/cm H2O
Convention dictations that “Compliance is reported between FRC and 1L above FRC”
Static Compliance
Compliance at no flow
Measured by consecutive oesophageal P measurements (which is surrogate for intrapleural P) & mouth P (when glottis is open mouth P = alv P)
∴getting your values for transpulmonary P = Alv P – Intrapl P
Maximal inspired breath
Breathe out into spirometer at 500mL increments
Small pauses to allow lung stabilisation
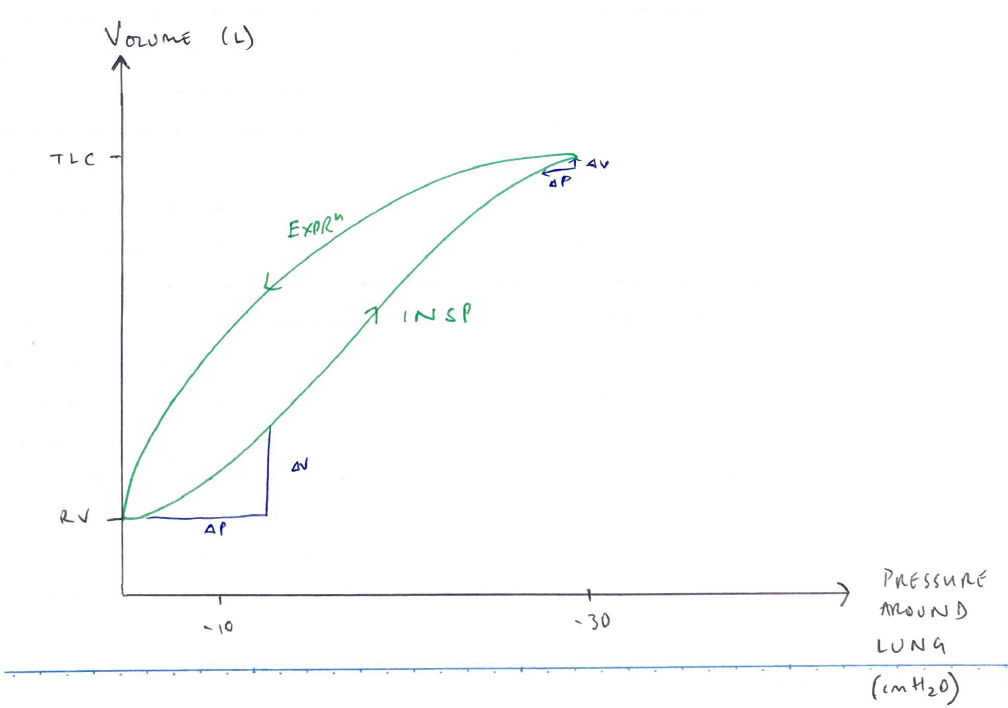
Plot curve P vs Vol
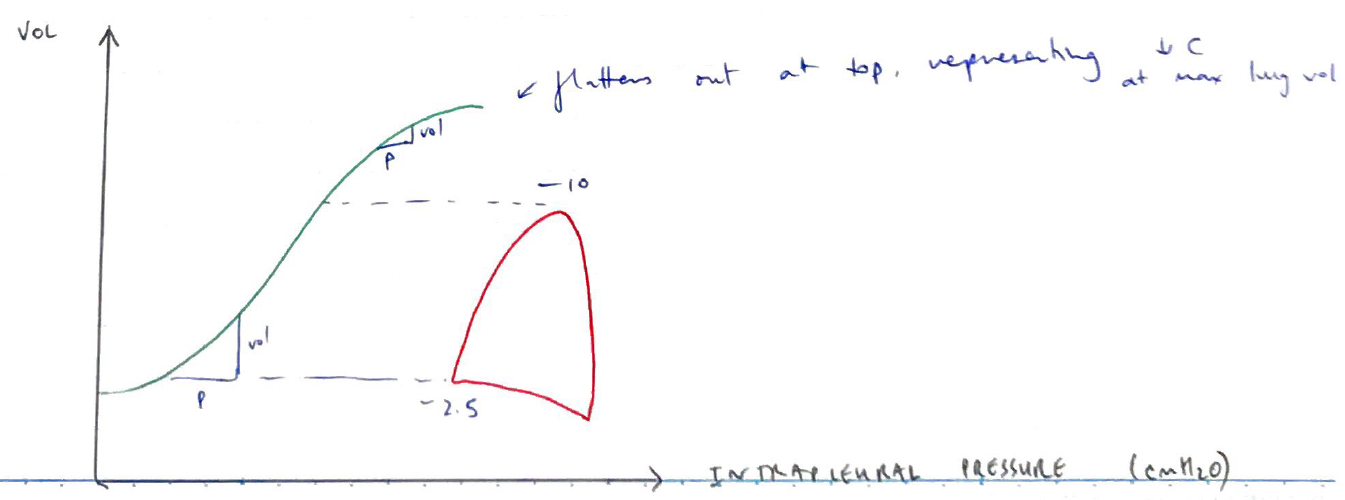
At low lung volumes, lung very distensible
At higher lung volumes, lungs reach limits of their distensibility
Dynamic Compliance
Compliance during respiratory cycle
Measured with Spirometry
Static compliance always > Dynamic compliance
Because you need greater P for the same volume ∆ because the resistive forces need to be overcome quicker
Also explains that ↑RR will ↓Dynamic compliance
Specific Compliance
Compliance / FRC = 0.05/cm H2O
Removes lung size so you can compare patients
Hysteresis
Compliance is less on INSP than EXPR
Occurs because on INSP you need more pressure to overcome ST forces & recruit additional alveoli