Outline the cardiovascular changes associated with morbid obesity (95% of marks).
23% of candidates passed this question.
This definition is straightforward and accounted for small proportion of marks.
A good answer discussed the key changes in the right and left heart, pulmonary, systemic and coronary circulation and changes to the cardiac conduction pathways. The underlying mechanisms for these changes because of morbid obesity were expected.
17A15: Exam Report
Outline the cardiovascular changes associated with morbid obesity.
42% of candidates passed this question.
Many candidates did not include enough detail in their answers.
Higher scoring answers included more depth such as the following: blood volume, left ventricular changes, arterial blood pressure, pulmonary artery pressures, risks of ischaemia, arrhythmias etc.
G6 / 25B12 / SYL2017 / 17A15: Outline the cardiovascular changes with morbid obesity
Definitions
Obesity = condition of excess body fat
BMI > 30kg/m2
CVS Consequences
HTN
X 10 more common
Multifactorial
↑blood vol → ↑CO → ↑BP
Hyperinsulinaemia → activates SNS → ↑Na+ reabsorption → BP
IHD
↑Cholesterol
HTN
DM
(Above are compounding factors)
NB:obesity is an independent RF for IHD
↑ Blood Volume & CO
Due to ↑metabolic demands of fat tissue
Extra blood vol is distributed to the fat tissue (cerebral & renal BF unchanged)
↑O2 consumption & CO2 production despite ↑CO
Cardiac Arrhythmias
Precipitation is multifactorial
Tissue hypertrophy/dilatation
Hypoxia
↓K+ from diuretics
CAD
↑Catecholamines
Fatty infiltration of conducting tissue
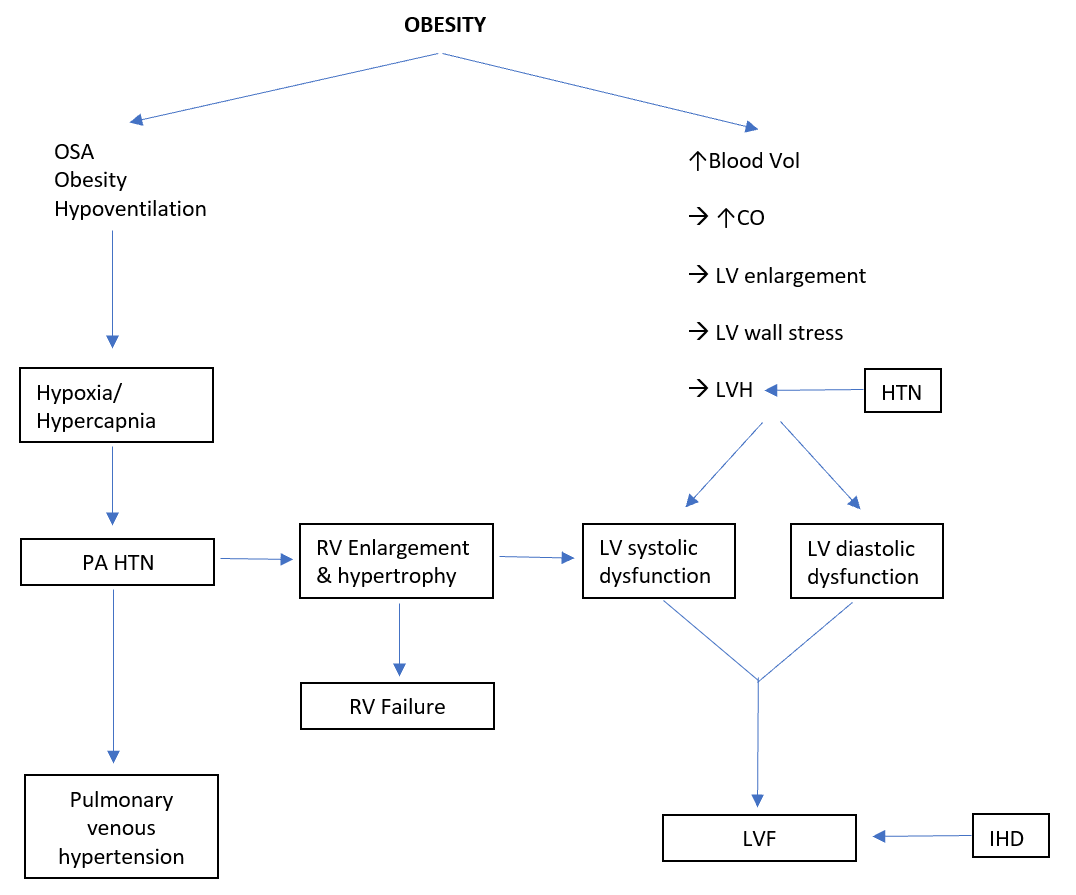
Cardiac Dysfunction
LVH
↑LV wall thickness & myocyte size
Hypertrophy to compensate for ↑CO
↑LV size & dilatation → ↑LV wall stress as per Law of LaPlace:
LV Systolic Dysfunction
↑Wall stress from LVH → contributes to systolic dysfunction