Describe how interstitial fluid recirculates to the vascular system.
10% of candidates passed this question.
Candidates had a limited understanding of this area of the syllabus. It was expected that answers would describe important concepts including the anatomy of venous structures, valves and lymphatics, permeability and factors which influence permeability. A description of hydrostatic forces, other pressures involved, and the role of osmotic and electric forces were required.
I1i / 17B04: Describe how interstitial fluid recirculates to the vascular system
Definition
Interstitial fluid is the fluid in the spaces between cells
Component of ECF
16% of total body weight
Fluid Filtration Across Capillaries
Fluid in the interstitium is derived by filtration and diffusion from capillaries
Fluid filtration across capillaries is determined by
Hydrostatic Pressures
Osmotic Pressures
Capillary Filtration Coefficient
Hydrostatic & oncotic pressures described by ∆ Starling Forces:
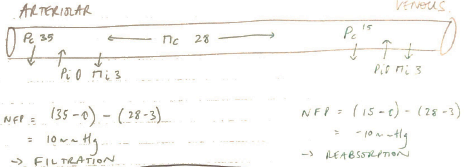
NET FILTRATION PRESSURE = Kf (PC – Pi) – s (πC – πi)
Kf = Filtration Coefficient
SA capillary walls x perm to H2O
e. a ‘leaky’ capillary due to histamine will have high Kf
σ = Reflection Coefficient
= Capillary permeability to proteins
This value ranges from 0 – 1
i.e. Hepatic sinusoids v. perm ~1
CSF & glomerular v. low closer to 0
Pc = Capillary Hydrostatic Pressure
Pushes fluid into interstitial space
Determined by arterial P, pre-cap & post-cap sphincter resistance
Pi= Interstitial Fluid Hydrostatic Pressure
Pushes fluid into capillary
ΠC = Capillary Oncotic Pressure
Generated by plasma albumin
Generates an osmotic force
Which prevents fluid moving out of capillary
Stable at 28mmHg through vessel length
Πi = Interstitial Fluid Oncotic Pressure
Generated by protein concentration of interstitial fluid
Promotes fluid movement out of capillary
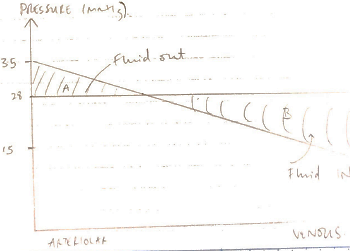
NFP is different at arterial & venous ends of caps
The fall in CAPILLARY HYDROSTATIC PRESSURE as blood flows from ARTERIAL à VENOUS end is responsible for the altered NFP
Fluid Loss
NET FLUID LOSS from filtration is 4L/day
This is all reabsorbed by lymphatics
Role of Lymphatic Circulation
Lymph = fluid which has entered lymphatic vessels from interstitial spaces
Anatomy
Lymphatic capillaries = everywhere EXCEPT CNS, bone & cartilage
Lymph vessels are blind-ending
Made of endothelial cells with a highly permeable BM
Possess flap valves between endothelial cells → permit one way entry of ISF
Lymph caps drain into larger lymph vessels
All lymph passes through LNs
Lymph returns to circulation via:
THORACIC DUCT → junction of L) subclavian & LIJ
R) LYMPHATIC DUCT → junction of R) subclavian & RIJ
Return of Fluid
Starling’s Forces result in:
Net Filtration ~20mL/min at arterial end
Net reabsorption ~18mL/min
∴2mL/min escapes into interstitium
This fluid is returned to circulation by lymph at a rate of 2mL/min (at rest)
Lymph Flow
Lymph flow 2mL/min (to return fluid from ISF)
EXTRINSIC & INTRINSIC factors promote this
Extrinsic: tissue pressure, skeletal m. activity, arterial pulsations → all compress lymph vessels
Intrinsic: smooth m. wall contraction in large lymph vessels & presence of 1-way-valves → ensure unidirectional flow
↑flow with exercise
If ISF volume > lymph drainage → OEDEMA
Interstitial Fluid Accumulation
Due to:
1. Imbalanced Starling Forces
↑PCg. fluid overload
↓πCg. malnutrition → ↓protein synthesis
↓Pig. negative pressure pulmonary oedema
↑πig. burns → plasma leak
2. Impaired Lymph Drainage
Lymphoedema due to LN clearance or blockage i.e. infection
3. Kf ↑ / ↑ σ
↑Kf with infection/inflammation = leaky caps
↑s in tissues with higher protein permeability i.e. liver