Compare and contrast two methods of measuring cardiac output.
35% of candidates passed this question.
Good answers began with a definition of cardiac output. For each method, it was expected that candidates discuss the theoretical basis, equipment, advantages and disadvantages / sources of error and limitations. Additional marks were awarded when an attempt was made to compare and contrast the two methods (often helped by the use of a table).
G6iii / 17B10: Compare and contrast two methods of measuring cardiac output
Cardiac Output
CO = HR x SV = volume of blood ejected by heart per minute
Determinants of CO are HR and SV
Techniques to Measure CO
Inavasive
Non Invasive
PAC
Dye Thermodilution
Fick Principle
TTE
TOE
Oesophageal Doppler
Pulse Contour Cardiac Output
PICCO
LiDCO
Partial CO2 rebreathing
Dye Thermodilution
Transoesophageal Echocardiography
Theory
CO measurement is based on the FICK PRINCIPLE
“Amount of indicator substance taken up over time = A – V difference of the substance x blood flow”
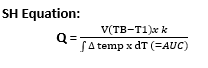
Current thermodilution practice of measuring CO uses a modified STEWART HAMILTON EQUATION
The marker is temperature
Uses Doppler technique to monitor cardiac function by multiplying the velocity-time integral (VTI) of blood flow through the transversal area of the vessel (CSA) with HR
CO = CSA * VTI * HR
Equipment
Thermistor-tipped Swan Ganz Catheter
Cold D5W
STEPS
Bolus of sterile solution (injectate) colder than pt blood is injected into RA port
Injectate mixes with RA blood → TV → RV → PA
Thermistor located 4cm from tip of catheter situated in PA detects ∆blood temp as blood passes catheter tip
Temp ∆ detected produces a curve which shows: ∆TEMP vs TIME calculated by a computer & converted into a measurement of CO by S – H application
Q = CO
V = volume of injectate
TB = temp blood
T1 = temp injectate
K = constant, which corrects for specific heat & density of inectate
dt = ∆ time
AuC is inversely related to CO
Small AuC = quick CO
Larger AuC = slow CO
Mean of 3 measurements is taken
Mean has to be 15% different to previous mean → otherwise there has been a margin of error
Transoesophageal ultrasound transducer
Skilled operator
Anaesthetised patient
The TOE probe is introduced into the mouth and passed down the oesophagus to visualise the Aortic Valve then inserted to the gastric cavity to obtain transgastric view of LVOT
Aortic Blood flow is obtained by pulsate Doppler
The VTIAORTIC os calculated by outlining the Aortic blood flow
Advantages
Non-toxic indicator
Repeated measurements easily
Computer performs all patented algorithms
Direct measurements in real time
Cardiac anatomy
Disadvantages
Associated w increased M&M:
Arterial injury
PTx
Chylothorax
Nerve injury
PA rupture
Valve damage
Risk of oesophageal perforation
Odynopahgia
Harmorrage
ETT malpositioning
Dental injury
Error/Limitation
Factors compromising technique:
Shunts
TR
Cardiac Arrythmias
Abnormal respiratory patterns
Low CO state
Assumes:
Constant flow
Normal heart & valves
No resp. fluctuations
Requires advanced training & expertise
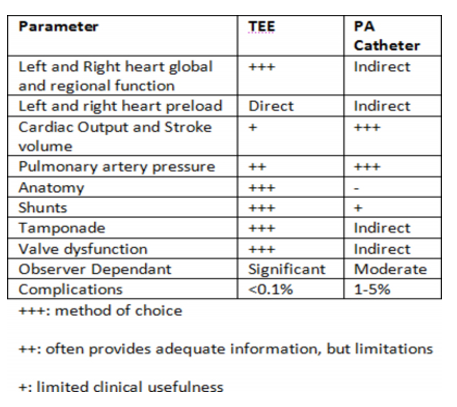
Comparison
PAC: constant PAP, frequent CO, sampling of SVO2 – however these values are modified by artificial ventilation and ventricular non compliance
TOE: gives direct measurements of values whereas PAC is indirect. Most PAC values can be calculated by TOE, except for SVO2
Safety: PAC has a higher complication rate (1-5% cf TOE 0.1-0.2%)