Describe the physiology of the NMDA (N-Methyl D-aspartate) receptor (40% of marks). Outline the pharmacology of ketamine (60% of marks).
49% of candidates passed this question.
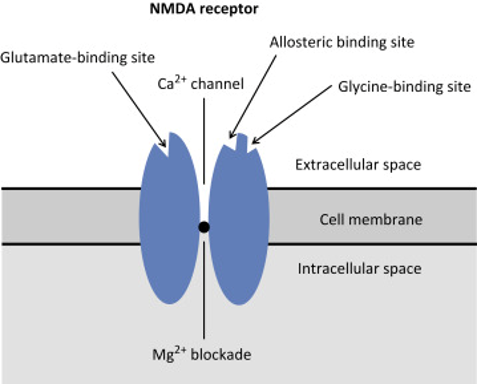
The NMDA receptor is a ligand gated voltage dependent ion channel located on post synaptic membranes throughout the CNS, with glutamate, an excitatory neurotransmitter, its natural ligand. A brief description of its structure, roles of glycine and magnesium, ions conducted, result of activation, role in memory and learning and agonists/antagonists was expected. Detail on structure and functions of the receptor were a common omission.
Ketamine, a phencyclidine derivative, is a non-competitive antagonist at the NMDA receptor. It is presented as a racemic mixture or as the single S(+) enantiomer (2-3 X potency). Administration routes and doses scored marks. Pharmacodynamics were generally well covered including CVS (direct and indirect effects), CNS (anaesthesia, analgesia, amnesia, delirium, effects on CBF and ICP) respiratory (bronchodilator with preservation of airway reflexes) GIT effects (salivation, N and V). Knowledge of specific pharmacokinetic parameters was less well covered, including low oral bioavailability and protein binding and active metabolite (norketamine).
K1vii / 19A15: Describe the physiology of the NMDA receptor (40 marks). Outline the pharmacology of Ketamine (60 marks)
Nmda Receptor
Definition: NMDA Receptors are ionotropic glutamate receptors
Structure
Heterotetramers
2 Glycine binding subunits
2 Glutamate binding subunits
Central pore
Located
Exclusively in neurons, widespread and expressed at post synaptic site
Function
Slow ESPS
Growth
Differentiation
Apoptosis
Synaptic Plasticity (Learning & Memory)
Excitotoxicity (ie pathophysiology of epilepsy, Alzheimer’s Disease)
Pain Sensitization:
Persistent pain will ↑[GLUTAMATE] & ↑signal transmission & causing Mg2+ dislodgement → NMDA receptor activates → CENTRAL SENSITISATION via 2nd messenger & further release of excitatory NT which ↑pain signal, even to benign stimuli
KA WIND UP
Endogenous Agonists
Glycine
Glutamate/Asparate (not as strong)
Ions Conducted
High Ca++ permeability
Na, K permeability
Result of Activation
Binding GLUTAMATE
Binding co-agonist GLYCINE
Membrane depolarisation (partial by other receptors AMPA & NK on some neurons)
↓
Mg2+ block released
↓
Na+, Ca2+ influx/K+ outflow
↓
Activation of protein kinase & phosphorylating enzymes