F4iv / 19B07: Closing Capacity
19B07: Exam Report
Define closing capacity (10% of marks). Describe the factors that alter it (30% of marks), its clinical significance (30% of marks) and one method of measuring it (30% of marks).
49% of candidates passed this question.
Many candidates confused the factors that affect closing capacity (CC) with factors which affect functional residual capacity (FRC). Some candidates confused airway closure with expiratory flow limitation secondary to dynamic airway compression.
A good answer would have included the following:
Small airway closure occurs because the elastic recoil of the lung overcomes the negative intrapleural pressure keeping the airway open. Thus, airway closure is more likely to occur in dependant parts of the lung where airways are smaller. Normally closing capacity is less than FRC in young adults but increases with age. Closing capacity becomes equal to FRC at age 44 in the supine position and equal to FRC at age 66 in the erect position. Closing capacity is increased in neonates because of their highly compliant chest wall and reduced ability to maintain negative intrathoracic pressures. In addition, neonates have lower lung compliance which favours alveolar closure. Closing capacity is also increased in subjects with peripheral airways disease due to the loss of radial traction keeping small airways open.
The consequences of airway closure during tidal breathing include shunt and hypoxaemia, gas trapping and reduced lung compliance. In addition, cyclic closure and opening of peripheral airways may result in injury to both alveoli and bronchioles. Closing volume (CV) may be measured by the single breath nitrogen washout test or by analysis of a tracer gas such as xenon during a slow exhaled vital capacity breath to residual volume. Residual volume (RV) cannot be measured directly but is calculated as follows: the FRC is measured using one of three methods: helium dilution, nitrogen washout or body plethysmography. The expiratory reserve volume (ERV) may be measured using standard spirometry. Using the measured FRC and ERV we may calculate RV from the equation:
RV = FRC – ERV. Then CC = RV + CV.
F4iv / 19B07: Define closing capacity (10 marks). Describe the factors that alter it (30 marks), its clinical significance (30 marks) and one method of measuring it (30 marks)
Definitions
- CC = lung volume at which the small airways in the lungs first start to close
- CC = closing volume + residual volume
- Closing vol = volume above RV at which small airways first start to close
Clinical Significance
- Small airway closure occurs because the elastic recoil of the lung overcomes the negative intrapleural pressure keeping airways open
- Weight of lung results in intrapleural P being less negative in dependent lung regions
- At low lung volumes intrapleural P at lung base may exceed atmospheric (airway P) → ∴ resulting in airway closure
- Airway closure → gas trapping
→ ∴blood flow through these non-ventilated areas → SHUNT
→ ↑a – A gradient
Factors That Alter It
Age
- Neonates: CC is high bc of highly compliant chest wall and reduced ability to maintain negative intrathoracic pressures ∴ more airways likely to collapse
- Young adults: FRC > CC
- 44yo supine: FRC = CC
- 66yo upright: FRC = CC
FRC → Position
- CC doesn’t ∆ with position, but FRC does
- ∴↓FRC with anaesthesia allows CC > FRC → A – a gradient ↑
Lung Pathology
- Chronic lung disease can ↑CC > FRC → ↑A – a gradient
Measurement
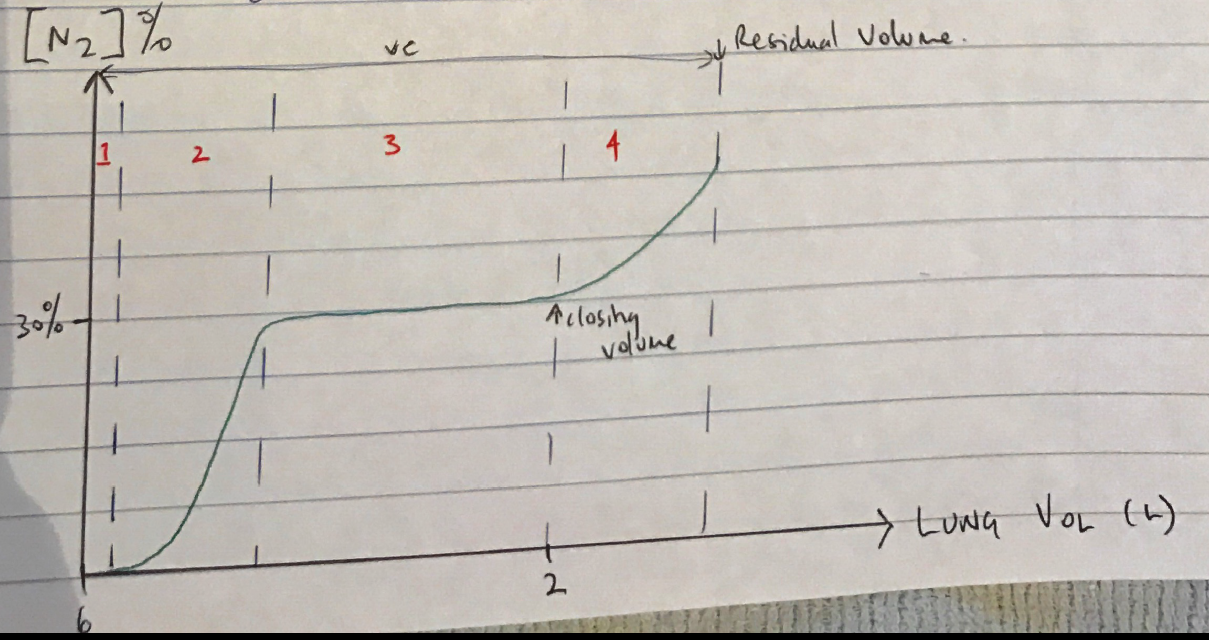
Single Breath N2 Washout
- Exploits topographical differences in ventilation to measure onset of small airway closure
- Subject takes VC breath breathing 100% FiO2
- N2 is measured on exhalation to produce 4 phases:
Ph 1: pure dead space exhaled
Ph 2: mixture dead space & alveolar gas
Ph 3: pure alveolar gas
Ph 4: at end of expiration abrupt ↑[N2] due to small airway closure → ∴what you’re measuring is preferential emptying of apical airways which have ↑[N2] because when the VC breath with 100% FiO2 was taken, the apex expanded less than the base
∴there was less N2 dilution with 100% O2
∴the volume at which small airways close can be used as CV
- Author: Krisoula Zahariou