Discuss the determinants of intracranial pressure (80% marks) and outline how it can be measured (20% marks)
64% of candidates passed this question.
In the good answers to this question, and there were a number, the candidates included the volumes of the cranium and a correct description of the Monroe Kellie doctrine.
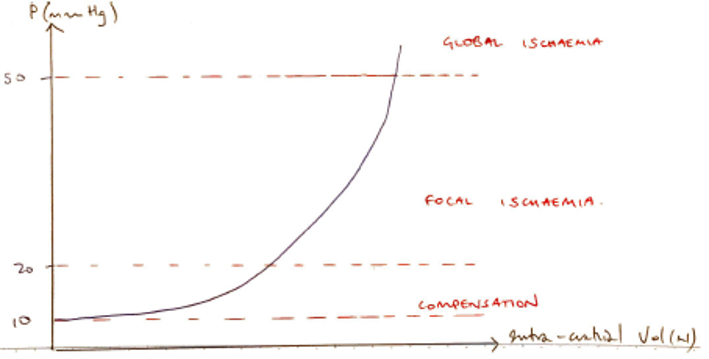
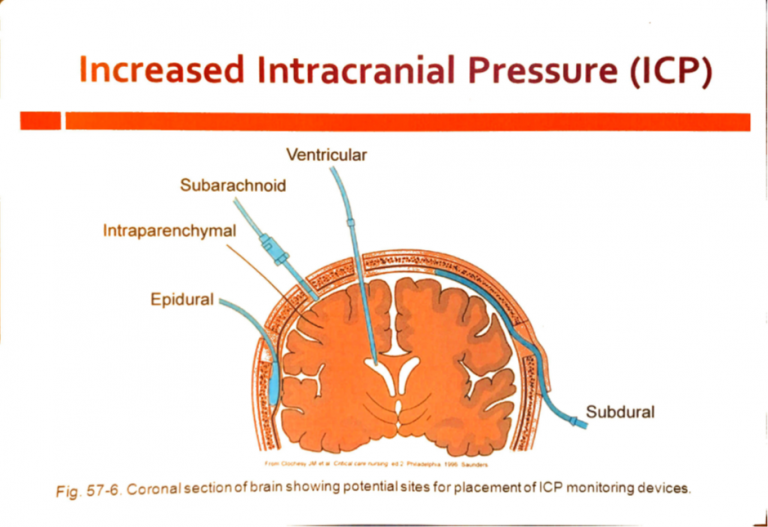
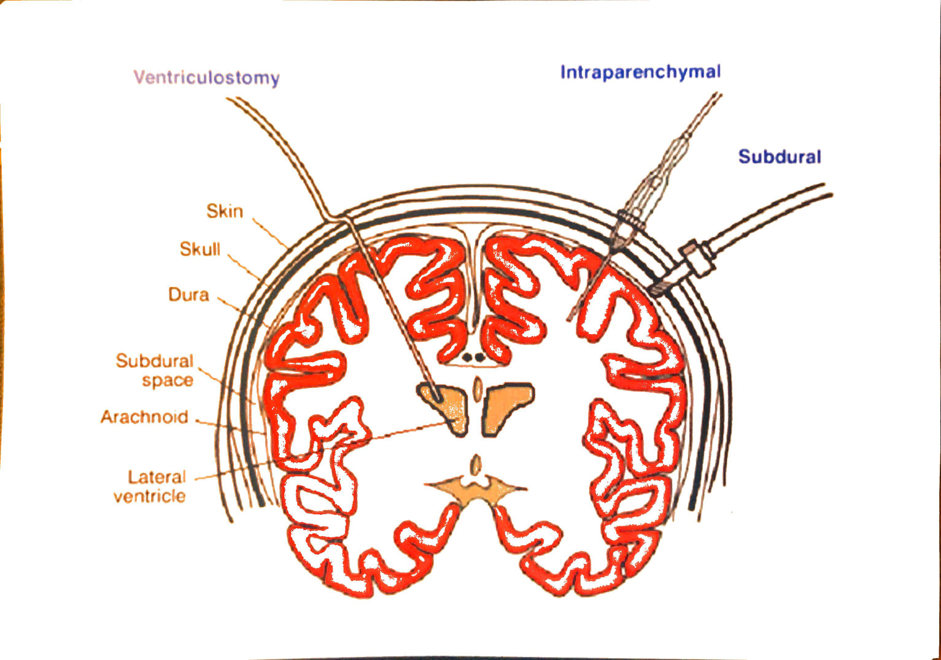
A good answer should have included the compensations and consequences of increases in intra-cranial volumes; a discussion of all three components (brain tissue, blood, and CSF) and how they affect intracranial pressure; and then information on intra-ventricular and parenchymal devices in measuring ICP, briefly including their pros and cons.
A common issue was writing quite a lot more than was needed on the relationship of cerebral blood flow to cerebral blood volume, and/or on the physiological consequences of raised ICP, which seemed to leave little time for discussion elsewhere.
A few candidates did not provide any response for ICP measurement (worth 20% of the marks). Few candidates provided the intra-cranial elastance equation. A significant proportion of candidates missed out a part of the question, either the factors that affect CBV or ICP measurement.
18A15: Exam Report
Describe the physiological regulation of intracranial pressure.
45% of candidates passed this question.
A definition and a normal value were expected. A description of the Monro-Kellie doctrine was expected. Better answers divided into the various components of the cranium with the answer focussing on cerebral blood volume and CSF volume as the brain tissue as no capacity to change its volume.
16B18: Exam Report
Discuss the determinants of intracranial pressure (80% of marks). Outline how it can be measured (20% of marks).
55% of candidates passed this question.
It was expected answers would include an explanation of the Monro-Kellie Doctrine. Many candidates gave insufficient details of compensatory mechanisms especially regarding decreased total cerebral blood volume (primarily venous) in response to increased intracranial pressure.
Most candidates had all the information but had difficulty synthesising the information to write a cohesive answer. Factors affecting ICP could be divided into factors affecting CBV, factors affecting CSF and factors affecting brain tissue. Under factors affecting CBV the effect of blood gases, autoregulation, temperature, metabolism, drugs and venous obstruction could have been detailed.
16A14: Exam Report
Describe the factors that influence intracranial pressure
69% of candidates passed this question.
A structure approached works well for “describe the factors …” questions. Better answers provided a definition of ICP, explained the Monro-Kellie doctrine and then detailed the factors which affect the volume of each of the components – cerebro spinal fluid (CSF), cerebral blood flow and brain parenchyma. Some candidates focused only on factors which cause intracranial hypertension and were thus unable to score full marks. Many candidates stated that CSF production was ICP dependant which is incorrect.
K1ii / 22A10 / 18A15 / 16B18 / 16A14 : Discuss the determinants of intracranial pressure (80 marks) + Outline how it can be measured (20 marks)
Definition & Normal Values
ICP = the pressure inside the cranial vault
Normal = 5 – 15mmHg
Determinants of ICP
Pressure inside fixed vault is exerted by a fixed volume of:
Brain tissue (80% volume)
CSF (5% volume)
Blood (10% volume)
ICP is determined by total volume of each
ICP also directly related to intrathoracic pressure as hit displays respiratory swing (ICP↑ coughing/straining/PEEP)
ICP is important because it determines CPP
CPP = MAP – ICP
Monroe-Kellie Doctrine
Skull is rigid box
Fluids are incompressible
M-K states that any ↑component of cranium must be met with equal ↓another component of cranium, for ICP to remain normal
Factors Affecting CBV
CBF = 750mL/min
CPP = MAP – CVP
An ↑ICP will create a Starling Resistor whereby ICP > CVP ∴CPP = MAP – ICP