Describe the sequence of haemostatic events following injury to a blood vessel wall until clot stabilisation
46% of candidates passed this question.
A good answer was well structured and covered the areas of vasoconstriction, platelet adhesion, activation and aggregation, coagulation, clot retraction and anticlotting mechanisms.
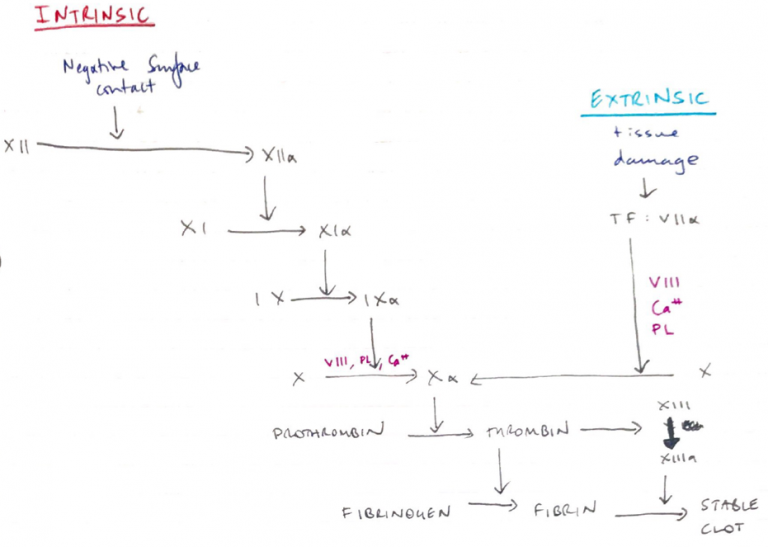
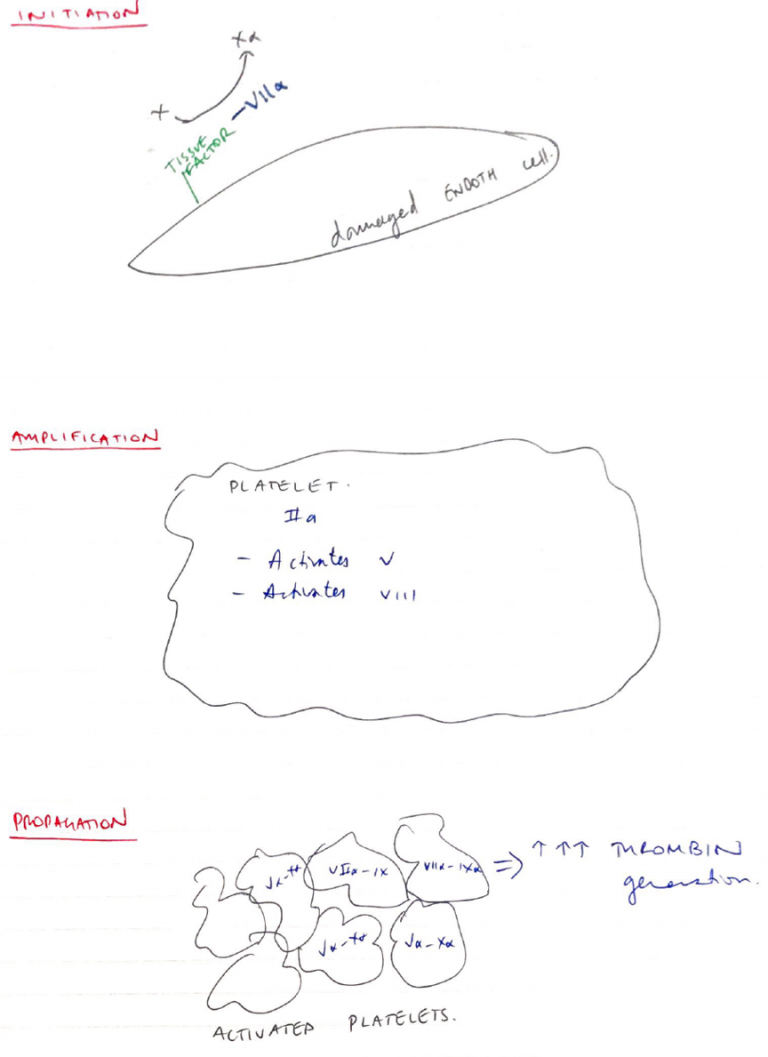
Many answers gave an overview of the haemostatic process but revealed insufficient knowledge of the processes involved. It was acceptable to give a classical view of clotting or to describe the cell-based model; or both.
However, in several cases answers became confused by mixing up elements of the classical approach and cell-based model approach. Errors concerning details of the cell-based model were frequent.
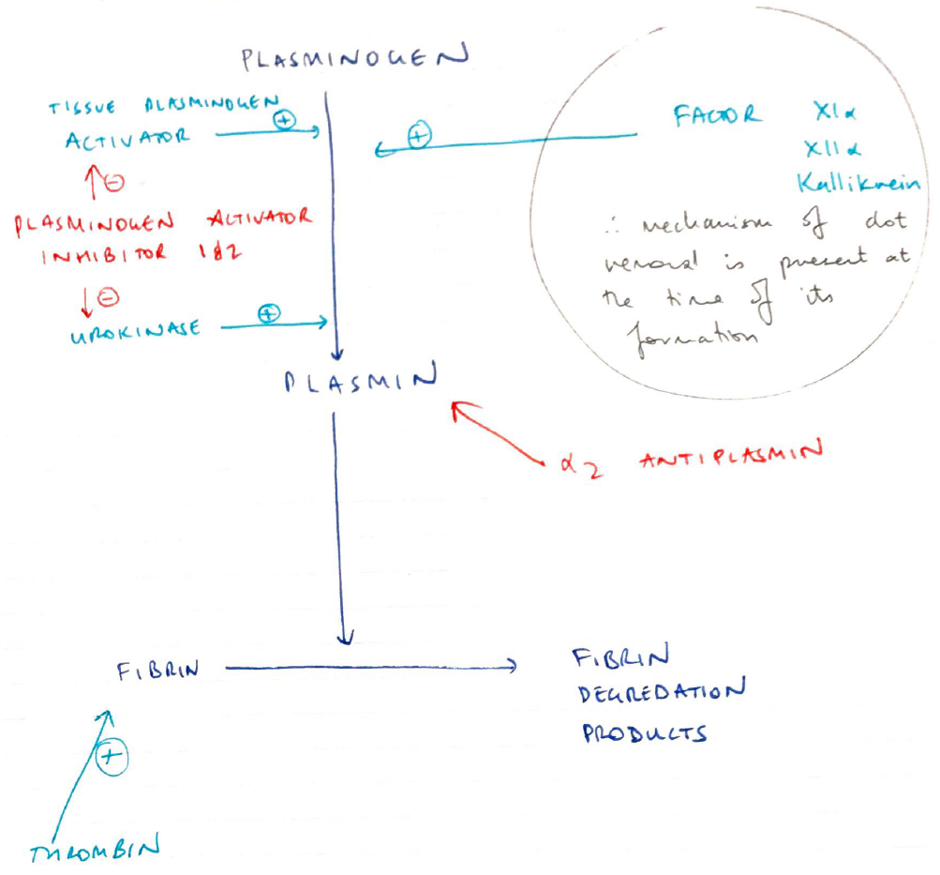
Many candidates did not include how the clot is limited to just the site of injury which happens in parallel with the formation of clot. Candidates should be aware that writing lengthy introductory statements attracted no marks and wastes time.
19A10: Exam Report
Outline the sequence of haemostatic events after injury to a blood vessel wall (50% of marks). Discuss the role of naturally occurring anticoagulants in preventing clot formation in-vivo (50% of marks).
40% of candidates passed this question.
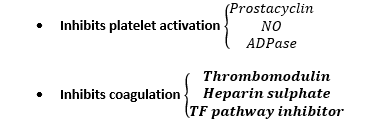
This question was best answered in a chronological manner. Many candidates omitted initial vasoconstriction and its mechanism. The platelet plug and formation of the clot should have then been described followed by the fate of the clot, including in-growth of fibroblasts. Strictly, fibrinolysis is a system for repairing / limiting clot propagation after the fact. Anticoagulants refer to antithrombin III, heparin, thrombomodulin and protein C and S. An explanation of the interaction of these naturally occurring anticoagulants was expected. The clotting factors that are specifically inhibited was expected as part of the discussion. The glycocalyx and vessel wall also plays a role in preventing coagulation.
Q1iv / 22A15 / 19A10: Outline the sequence of haemostatic events after injury to a blood vessel wall (50 marks). Discuss the role of naturally occurring anticoagulants in preventing clot formation in-vivo (50 marks).
Haemostasis
Haemostasis = cessation of bleeding
3 Steps
PRIMARY HAEMOSTASIS = platelet plug formation
SECONDARY HAEMOSTASIS = coagulation to form FIBRIN MESH (which reinforces platelet plug)
FIBRINOLYSIS & VESSEL REPAIR
Vascular Endothelium
Coated with GLYCOCALYX & BM (= intima layer)
Glycocalyx = complex gel of glycoproteins & proteoglycans that is produced by & coats endothelium
Intact blood vessel provides non-thrombogenic surface that blood can pass through circulatory system