H1iv / 23B03 / 22B07: Describe the physiological mechanisms by which the kidney is able to concentrate urine
23B03: Exam Report
Describe the physiological mechanisms by which the kidney is able to concentrate urine
52% of candidates passed this question.
This question required the identification of the components of the kidneys function that work to concentrate urine and a detailed description of how each of these components contribute to this.
These components included the role of the loop of henle and vasa recta in the establishment and maintenance of the medullary osmotic gradient, the contribution of urea and urea cycling to this gradient and the subsequent contribution of antidiuretic hormone.
A focus on not how urine is formed but how it is concentrated was expected.
22B07: Exam Report
Describe the physiological mechanisms by which the kidney is able to concentrate urine
35% of candidates passed this question.
Answering this question well required the demonstration of understanding of the concept of achieving maximum urinary concentrating ability.
Answers required a description of the usual concentrating processes and the changes that would occur in circumstances where maximally concentrated urine would be made.
A key concept was the creation of a medullary concentration gradient to allow water reabsorption independent of solute reabsorption.
This required an explanation of the contribution of the loop of Henle, the vasa recta, and urea cycling in the creation and maintenance of this gradient, along with the impact of ADH.
More detailed explanation of each contribution was required as overarching statements were not sufficient to attract all marks for each section.
Answers that focused solely on the counter-current exchange and multiplier process were insufficient on their own to achieve a passing mark.
The examiners commented that a significant proportion of candidates excluded the role of urea in their answers.
H1iv / 23B03 / 22B07: Describe the physiological mechanisms by which the kidney is able to concentrate urine
Introduction
The kidneys ability to concentrate urine depends on the following processes:
- Countercurrent multiplier of loop of henle
- Urea recycling
- ADH
- Vasa recta
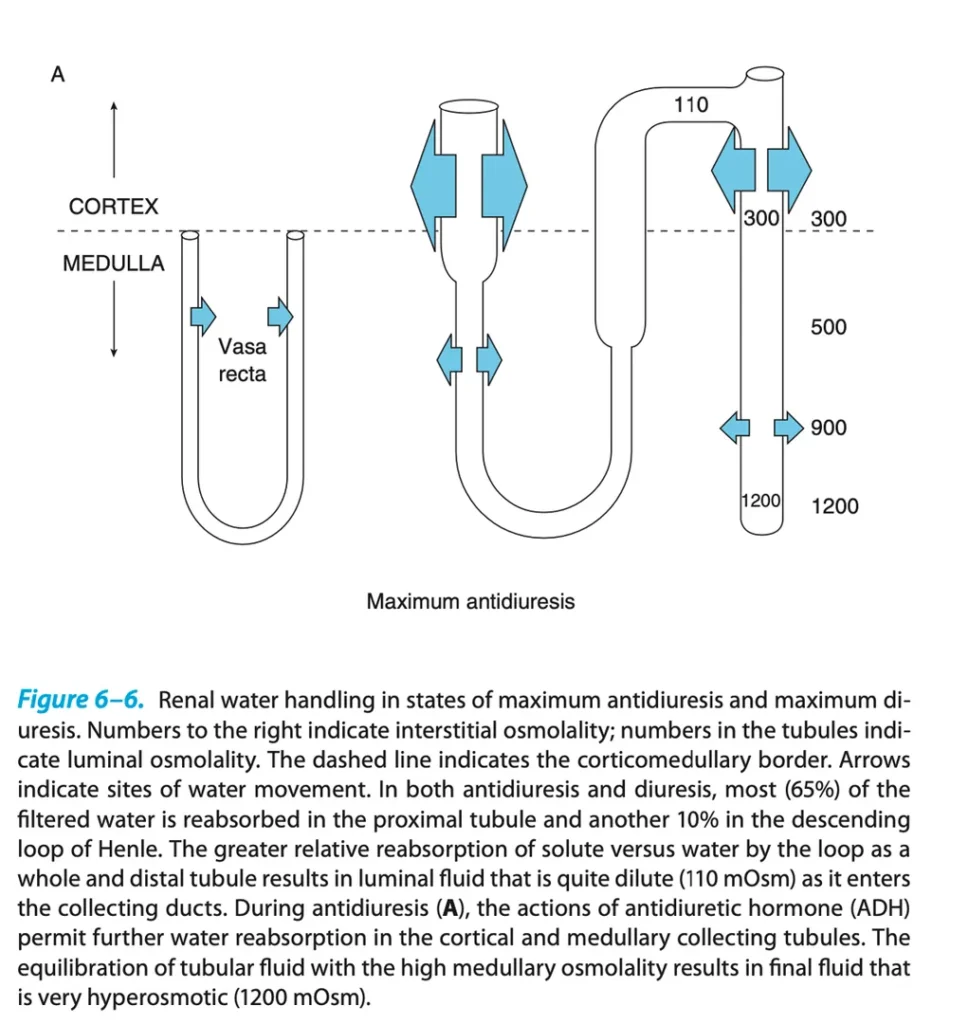
Maximally concentrated urine
- Maximally concentrated (hyperosmotic) urine Osmolality is 1400mOsm/kg,
- Minimal urinary volume is 430ml per 24 hours to clear 600mOsm solutes = obligatory water loss
- To produce maximally concentrated urine, almost all (>99%) filtered water is reabsorbed: 65% In PCT, 10% in thin descending limb of loop of Henle, and >24% in collecting duct system.
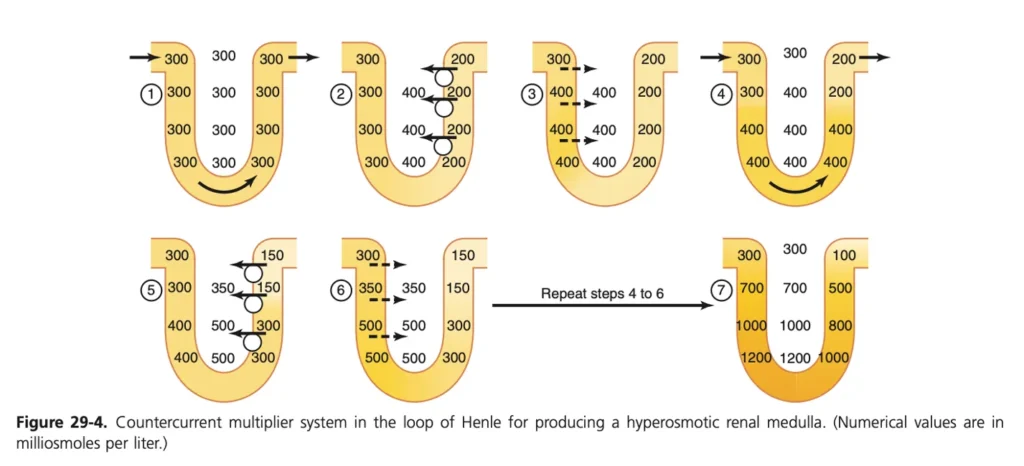
Countercurrent multiplier
- An interstitial osmotic gradient is generated in the renal medulla by the action of the countercurrent multiplier in the loop of Henle
- This countercurrent multiplier aids in generation of concentrated urine because it allows maximal water reabsorption from the collecting duct, in the presence of ADH
- The countercurrent multiplier works as follows:
- The descending limb epithelium is permeable to water but not solute
- The thin ascending limb is passively permeable to solute, and impermeable to water
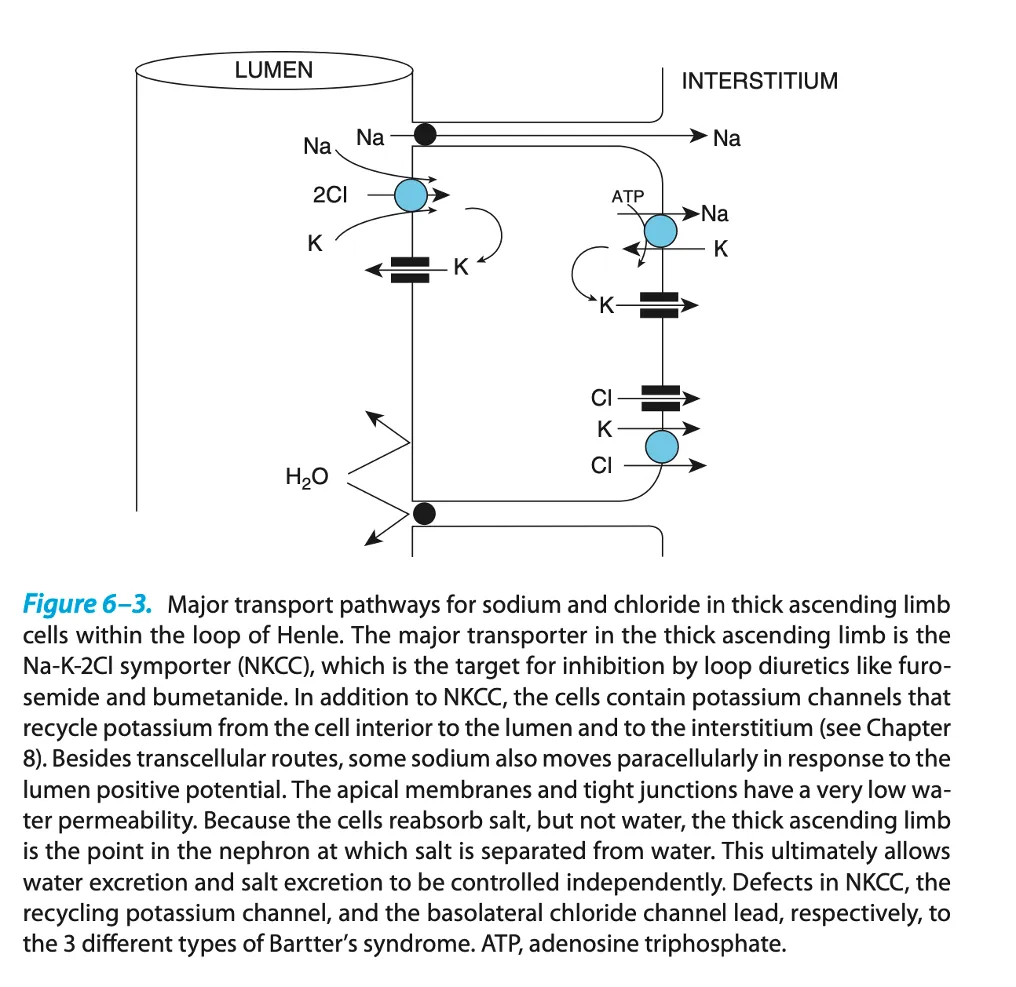
- The thick ascending limb actively pumps solute out of the filtrate and into the intersitium, and is impermeable to water. The active pumps on the apical membrane are Na/K/2Cl cotransports and Na/K ATPases on the basolateral membrane, as well as Cl channels on the basolateral membrane (Fig 6.3)
- This means, as filtrate from the DCT passes through the loop (Osm 300mOsm/kg), 100mOsm/kg of solute is actively reabsorbed
- This means the Osmolarlty in the interstitium increases
- This causes water to leave the descending limb via osmosis
- This causes the Osmolality of the filtrate in the descending limb to increase to 400mOsm/kg
- This filtrate then flows through from the descending limb to the ascending limb and the cycle repeats
- This causes a progressive increase in the interstitial osmolality with a gradient increasing from iso-osmotic at the corticomedullary border, to hyperosmotic ~1200mOsm/kg at the papilla (Fig 29.4)
- Due to low blood flow in the medullary interstitium, this solute is not immediately reabsorbed which allows the gradient to be generated
Urea recycling
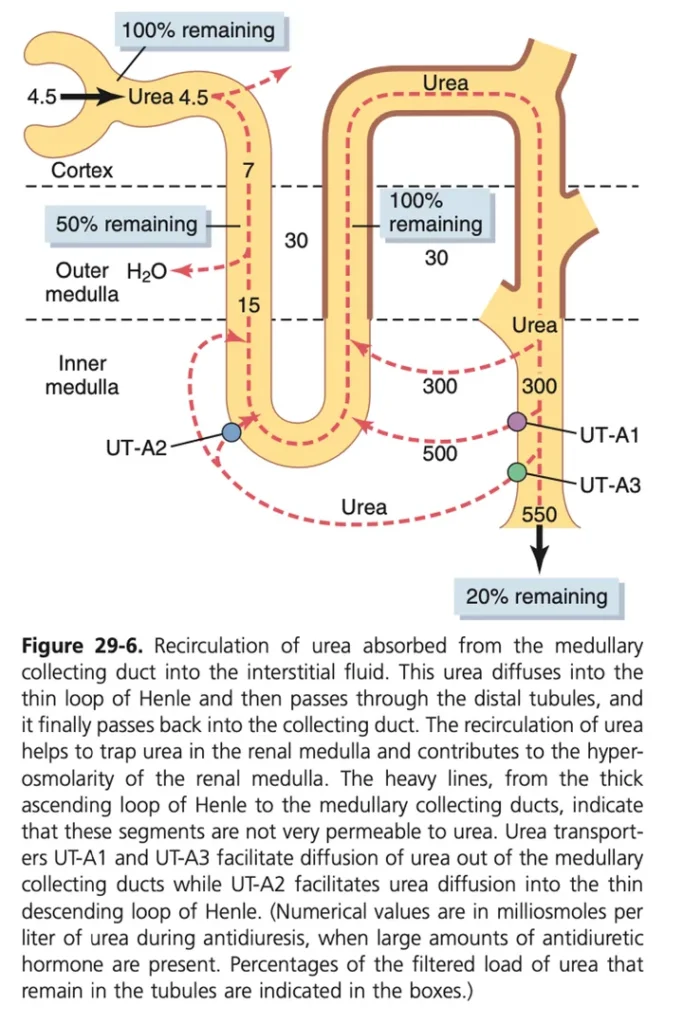
- Urea is freely filtered at the glomerulus (900mmol/day)
- 50% is reabsorbed in the PCT. Most of the tubular system is impermeable to urea.
- As water is reabsorbed from the cortical and outer medullary collecting ducts, this increases the concentration of urea within the filtrate to very high levels (>500mmol/L)
- In the presence of ADH; urea transporters UT-1 and UT-3 are inserted into the inner medullary interstitium.
- This causes reabsorption of urea into medullary interstitium, which increases the osmolality of the interstitium, and contributes up to 50% of the gradient.
- Because blood flow to the medullary interstitium is low, the urea concentrates to a similar concentration within the filtrate (>500mmol/L).
- Urea is then secreted into the thin limbs of loop of Henle (driven by the high urea concentration in the medullary interstitium)
- This reabsorption of urea in the presence of ADH aids generation of maximally concentrated urine, because it maintains the medullary interstitial osmotic gradient despite water reabsorption from the collecting duct
Impact of ADH
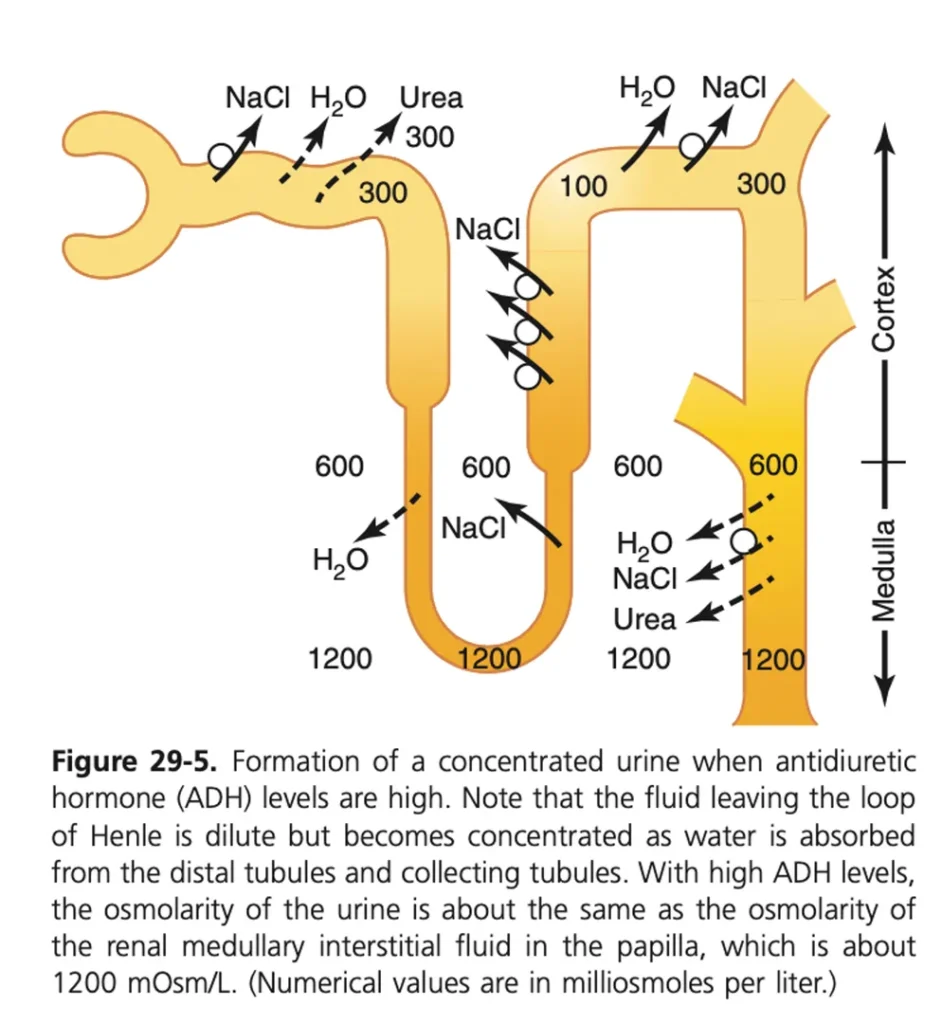
- ADH is required to produce maximally concentrated urine
- It acts on the V2 receptors on the basolateral membrane of principle cells of the medullary and cortical collecting duct cells to cause insertion of apical AQ2 channels from intracellular vesicles (via Adenylyl Cyclase, cAMP dependant), which cause water reabsorption
- The basolateral membrane already contains aquaporin channels, so insertion of AQ2 channels into the apical membrane ultimately leads to water reabsorption across the cell into the interstitium.
- The generation of the medullary interstitial concentration gradient via countercurrent mechanism, and maintenance of the gradient via urea cycling are fundamental to allow the insertion of these channels to lead to maximal water reabsorption and therefore maximal urine concentration
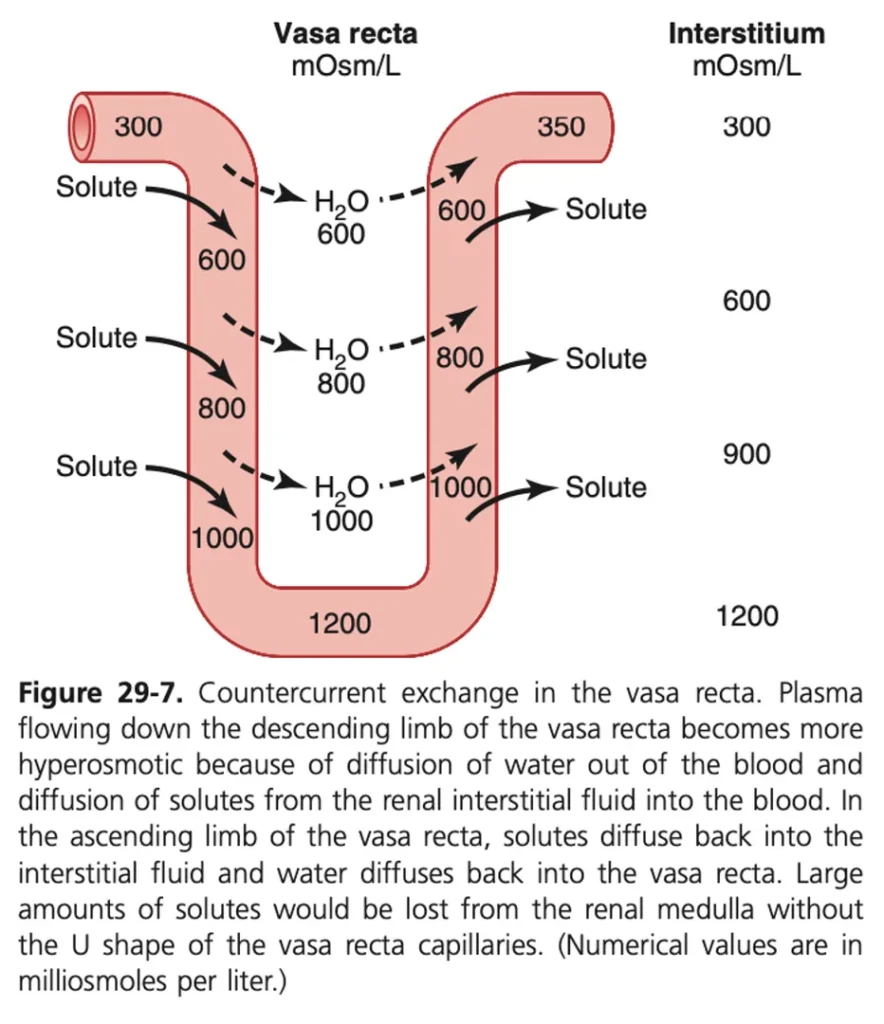
The vasa recta
- Vasa recta are important in the production of concentrated urine because they allow passive solute and water reabsorption without disrupting the medullary interstitial osmotic gradient, and therefore allow the continued maximal water reabsorption from the collecting ducts.
- This occurs because the vasa recta are low flow, and run as loops with descending and ascending limbs in close association.
- This allows countercurrent exchange between the descending and ascending limbs, preventing dilution of the intersitium.
- As the descending limb of the vasa recta flows into the inner medulla, it absorbs solute and loses water to the interstitium. The ascending limb then absorbs water and loses solute.
- This means some solute and water can be absorbed without diluting the gradient. The osmolality of blood entering the loop is ~300mOsm/kg and the osmolality exiting is ~320mOsm/kg.
Author: Alex Ashby