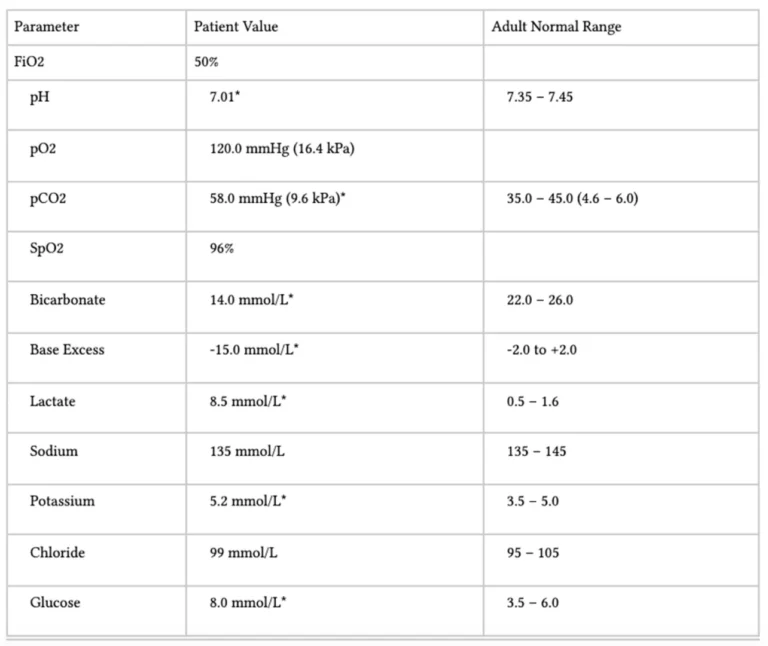
Outline the abnormalities in the following arterial blood gas (25% of Marks). Explain the Stewart approach to acid-base interpretation (75% of Marks)
21% of candidates passed this question.
High performing answers correctly outlined the ABG findings including consideration of electrolyte abnormalities, A-a gradient, acid-base disturbance (including anion gap and strong ion difference) and whether compensation was appropriate.
The best explanations of the Stewart approach described its physicochemical basis, discussed the independent variables (strong ions, total weak acids, and pCO2) in detail, and described their effect on the dependent variables and how they result in acid-base derangements.
The ABG provided depicted an incorrect base excess with an omission of (-) symbol.
Candidates were marked accordingly depending on their response to this and all candidates were compensated equally for the confusion that this may have caused.
J2i / 23A01: Outline the abnormalities in the following arterial blood gas (25% of Marks). Explain the Stewart approach to acid-base interpretation (75% of Marks)
Interpretation of ABG
An approach to ABG analysis….(find an approach and stick to it – I like Deranged’s)
This is an example ABG and not the ABG on the actual exam paper
1. A-a gradient: calculate
PAO2 = (FiO2 x 713) – (PaCO2 x 1.25)
(expected) PAO2 = (0.5 x 713) – (58 x 1.25) = 356 – 72.5 = 283
(actual) PaO2 = 120
A-a = 283 – 120 = 163
Normal A-a gradient = 10mmHgh +1mmHg for every decade of life
Therefore there is a raised A-a gradient (you need to show the working to gain marks)
2. Describe the pH change:
Acidaemia / Alkalaemia
3. What is the Base Excess Change:
HCO3
1mmol increase w Acute Respiratory Acidosis
4mmol increase w Chronic Respiratory Acidosis
2mmol decrease w Acute Respiratory Alkalosis
5mmol decrease w Acute Respiratory Alkalosis
CO2
For Metabolic Acidosis: PaCO2 = (1.5 x HCO3) + 8
For Metabolic Alkalosis: PaCO2 = (0.7 x HCO3) + 20
Metabolic Acidosis
ePaCO2 = (1.5 x HCO3) + 8
ePaCO2 = (1.5 x 14) + 8
ePaCO2 = 29
aPaCO2 = 58
Therefore there is inadequate compensation and a Respiratory Acidosis as well
5. Anion Gap:
Calculated to evaluate the cause for metabolic acidosis & determine the presence of unmeasured anions
Normal AG = 4-12
NAGMA (USED CRAP)
Ureteric Diversion
SB fistula
Extra Chloride
DKA
CA Inhibitors
Addisons
RTA 1,2,4
Pancreatic Fistula
HAGMA (L TKR)
Lactate
Toxins
Ketones
Renal (failure to excrete organic anions Sulphate, Hippurate, Phosphate)
AG = Na – (Cl + HCO3)
AG = 22
Therefore there is a raised Anion Gap Metabolic Acidosis
6. Mention other glaring abnormalities
Make a comment on the electrolytes/glucose/albumin etc if they are given
Hyperlactaemia which is contributing to the HAGMA
Stewart Approach
Introduction
AKA Physiochemical Approach
Differs from HH which is determined by H+ & HCO3–
3 independent variables which control acidity
Independent Variables → these ∆ pH (= 1° cause)
pCO2
ATOT (total weak non-volatile acids)
SID
Dependent Variables (= 2° effect)
These values depend on values of independent variables
If these ∆, then independent variables must have ∆
H+
OH–
CO32-
HA (weak acid)
A–(weak anions)
Physical Laws Of Physiochemical Methods
Interaction of dependent & independent variables must obey the laws of aqueous solution:
ELECTRONEUTRALITY – in any aqueous solution the sum of all +vely charged ions must equal the sum of all -vely charged ions
DISSOCIATION EQUILIBRIA – derived from Law of Mass Action. The velocity of a chemical reaction is proportional to the active [ ] of the reaction
CONSERVATION OF MASS – the amount of substance remains constant unless added, removed, generated, or destroyed
Strong Ions
Definition = ions that completely dissociation in a solution
SID of H2O
H2O → H+ + OH–
Determined by SID
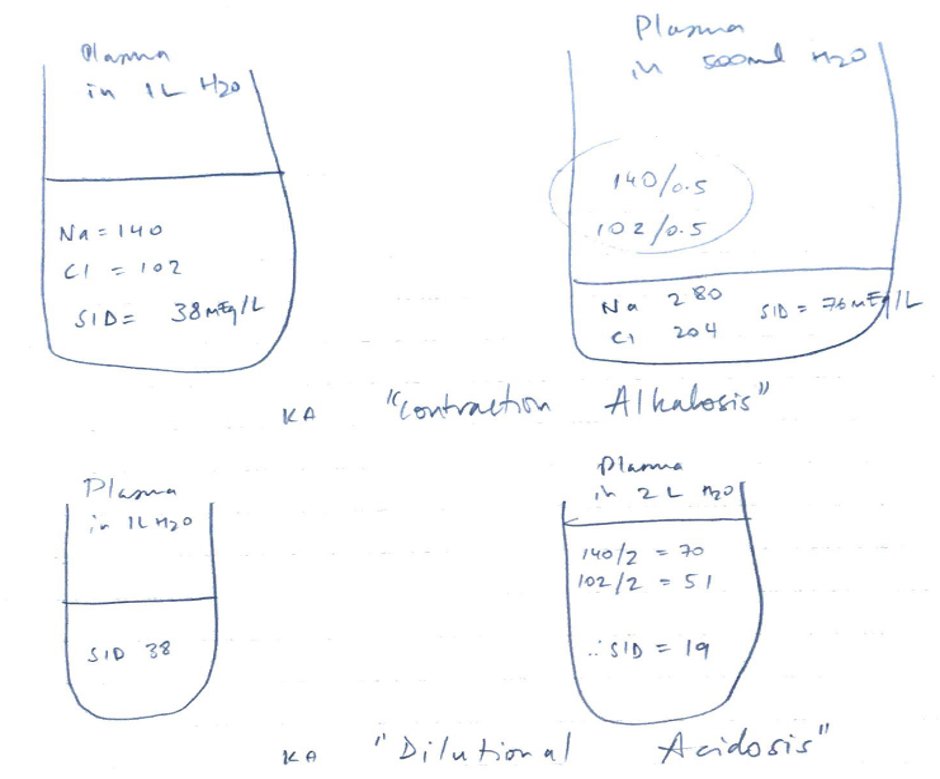
SID= [strong cations] – [strong anions]
↑OH– = alkalosis
↓OH– = acidosis
Recall: H2O → OH– + H+because altering OH– will alter H+(dissociated)
SID in Plasma
All solutions of body have H2O
[H+] of these solutions depends on the dissociation of H2O
H2O dissociation depends on the VARIABLES!
SID, PCO2, ATOT
Strong cations = Na, K, Ca, Mg
Strong anions = Cl, SO42-
SID = strong cations – strong anions
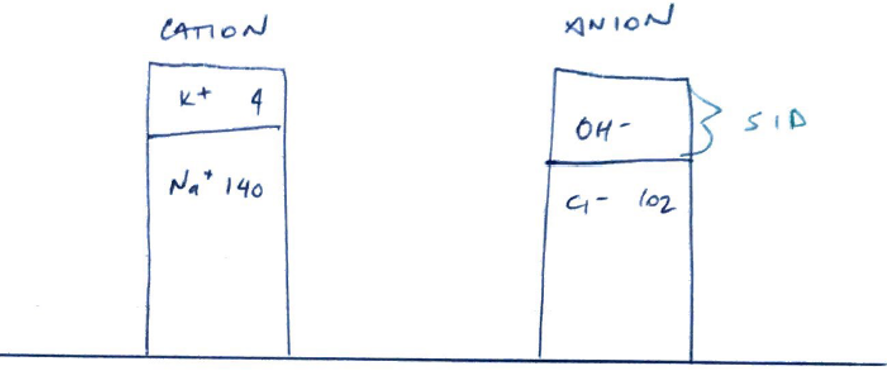
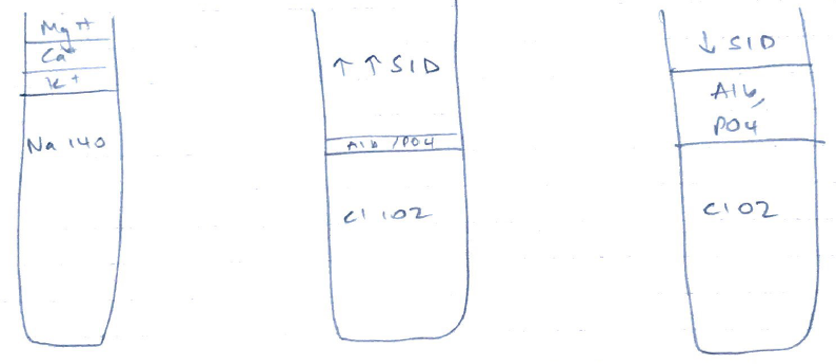
Normal plasma SID = 42 mEq/L
But you must have Electroneutrality
Whereby Anions = cations so that the SID = 0
But it’s not, it’s 42mEq/L and slightly alkaline
∴somewhere in plasma is unmeasured anions (the OH- in the above gamblegram)
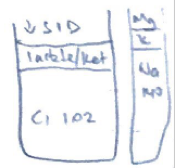
↑SID = alkalosis (the unmeasured anions have increased further)
↓SID = acidosis (there are less unmeasured anions)