G7iii / 23A11: Outline the Vaughan Williams classification of anti-arhythmic drugs with examples (30% of Marks). Describe the relevant pharmacology of adenosine (70% of Marks)
23A11: Exam Report
Outline the Vaughan Williams classification of anti-arhythmic drugs with examples (30% of Marks). Describe the relevant pharmacology of adenosine (70% of Marks)
67% of candidates passed this question.
The high pass rate of this question was largely due to the ability of most candidates to reproduce the VW classification, with correct information regarding each class with examples.
The pharmacology of adenosine was less consistently covered and whilst most kept to the usual pharmacology structure correct detail was often lacking to achieve high marks for this section.
G7iii / 23A11: Outline the Vaughan Williams classification of anti-arhythmic drugs with examples (30% of Marks). Describe the relevant pharmacology of adenosine (70% of Marks)
V – W classify antiarrhythmic in groups based on electrophysiological characteristics → based on micro-electrode studies
Class
I
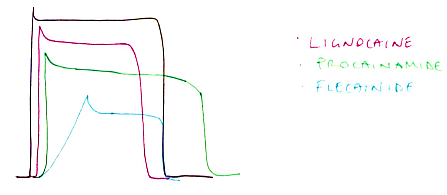
SODIUM CHANNEL BLOCKERS
Example
IA – PROCAINAMIDE
IB – LIGNOCAINE
IC – FLECAINIDE
Mechanism of Action
Moderate Na+ channel block, ↑refractory period
Weak Na+ channel block, shortens AP
Strong Na+ channel block, no effect refractory period
Class
II
β-BLOCKERS
Non-selective
Selective
Intrinsic sympathomimetic activity
Example
PROPANOLOL
METOPROLOL
LABETALOL
Mechanism of Action
Antagonises effects of catecholamines at β receptors
In heart: – CHRONO, – DROMO, -INOTROPY
↓slope Ph 4 = more time to reach threshold = ↓discharge rate
Class
III
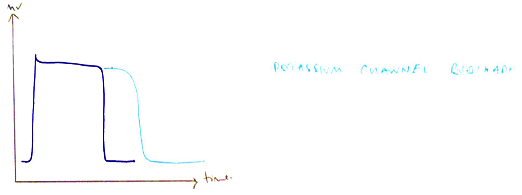
POTASSIUM CHANNEL BLOCKERS
Example
AMIODARONE
SOTALOL
Mechanism of Action
Blocks K+ channels
Prolongs refractory period of all cardiac time
Broad spectrum: blocks Na+ channel, K+ channel, Ca2+ channel & α + β adrenoreceptors
Class
IV
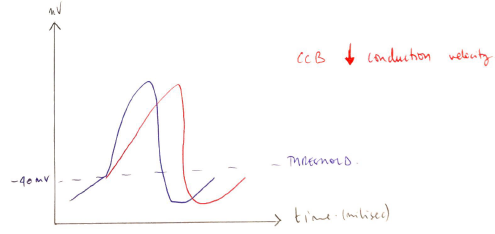
CALCIUM CHANNEL BLOCKERS
Example
DIHYDROPYRIDINES
BENZOTHIAPINES
PHENYLALKYLAMINES
Mechanism of Action
→ NIMODIPINE → Block Ca2+ channel of arteries
→ DILTIAZEM → AV node → inhibits inward Ca2+ current (↓rate conduction AV node)
→ VERAPAMIL → AV node → inhibits inward Ca2+ current (↓rate conduction AV node)
Class
OTHER
Example
Mechanism of Action
DIGOXIN
- Activates vagal nuclei = ↑ activity
- Inhibits Na/K/ATPase = RMP becomes less negative 2° ↑intrac. K (depol easier); AP shortens 2° ↑K conduction
ADENOSINE
A1 receptor on SA node → stimulates adenosine sensitive K+ channel → ↑K conductance = hyperpolarises – VE DROMOTROPY
MAGNESIUM
- Co-factor Na/K/ATPase
- L-type Ca2+ channel antagonist ECG prolongs R:R, ↑PR interval
- ↑AV conduction time
Sodium Channel Blockers
- Inhibit Fast Na+ channel of fast AP cells
- ↓slope of Ph 0
- ↓amplitude AP
- ↓conduction velocity (negative dromotrope) so that there is slower transmission of AP
→ Subdivided based on duration of AP (effect on refractory period)
IA – Procainamide
- Moderate Na channel block
- ↑refractory period → lengthens AP
IB – Lignocaine
- Weak Na+ channel block
- Shortens AP
IC – Flecainide
- Strong Na+ channel block
- No effect refractory period
Na+ channel block: IC > IA > IB
Lengthen AP: IA > IC > IB (decreases)
Beta Blockers
- Competitive antagonists of β1/β2 adrenoreceptors
- Antagonise effects of catecholamines
- ↓slope of Ph 4 = more time to reach threshold = ↓discharge rate
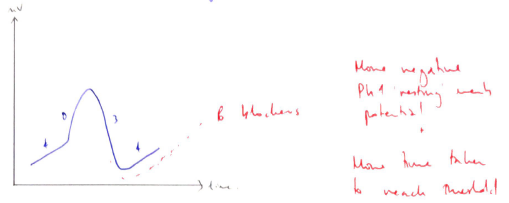
- – VE CHRONO, DROMO, INOTROPY
↓myocardial O2 consumption
Potassium Channel Blockers
- Block K+ channels responsible for repolarisation
- Prolong AP
- This ↑effective refractory period
- On ECG → prolongs QT interval
Calcium Channel Blockers
- Class 4 antiarrhythmics
- Diverse & structurally unrelated
- All block Ca2+ channels
- Classified on basis of CHEMICAL STRUCTURE
Dihydropyridines → Nimodipine
- Block Ca2+ channel of peripheral arteries
- Via extracellular modulation of Ca2+ channel
- Prevents Ca2+ entry into smooth m. cell
Benzothiapines → Diltiazem
- Intermediate between the other 2
- Predominate effect = AV NODE
- Inhibits inward Ca2+ current
- ↓rate conduction of AV Node → ↑PR interval
Phenylalkylamines → Verapamil
- Predominant AV Node, SA Node
- Physically occludes Ca2+ channel
- ↓rate conduction → ↑PR interval
Adenosine
Adenosine
Chemical
An endogenous nucleotide present in all metabolising cells
Made of a purine base (adenine) & a sugar (ribose)
Use
- SVTs
- Differentiate flutter & SVT
Presentation
Clear, colourless solution 3mg/mL
Dose
(IV) 6mg → 12mg at q2mins
Give as centrally as possible with rapid flush
Route
IV
Onset
Rapid, needs to be flushed
OFFSET:
- Rapid t ½ 10 secs
Deaminated to INOSINE + AMP in plasma or taken up by RBC
MoA (mechanism)
Agonist of adenosine receptors
Receptor
A1
SA Node
Atrium
Messenger
- Gi
↓
Inhibits AC
↓
cAMP
↓
↓Ca2+
- Stimulates adenosine sensitive K+ channels
↓
↑K+ conductance
↓
Hyperpolarises supraventricular myocytes
Effect
↓Ca2+ influx = negative INOTROPY
Inhibition of AV conduction = negative DROMOTROPY
Receptor
A2
Smooth muscle of arteries & coronary arteries!
Messenger
- G5
↓
Activates AC
↓
↑cAMP
↓
Inhibits M1CK
↓
Relaxes smooth m.
Effect
Vasodilation
↑coronary BF
ECG effects: ↓HR
PD
CVS
- AV block à slows ventricular response
→ Terminates SVT
→ Reveals atrial arrythmia
RESP
- ↑MV
- A2 receptors of carotid body stimulated
CNS – ↑CBF
Metabolic – stimulates glycolysis
PK
A
Inactivated orally
D
Quick 10s t½
Needs to be followed by rapid IV bolus
M
Deaminated to INOSINE + AMP in plasma or taken up by RBC
E
Taken up by RBC
t ½ 10 secs
Adverse Effects
- Transient flushing
- Dyspnoea, bronchospasm
- Chest discomfort
- Profound bradycardia requiring pacing