Explain how the kidneys handle glucose (70% of marks).
Outline the renal consequences of glycosuria (30% of marks).
45% of candidates passed this question.
The expected information in this question included discussion of the sites at which glucose transport occurs (primarily glomerulus and proximal convoluted tubule) and the transport mechanisms involved including specific transporters. A discussion of the maximum transport concept was also required.
This section required a discussion of the glucose induced osmotic diuresis and subsequent electrolyte loss. Additional marks were available for answers which recognised that this diuresis was not able to be overcome by ADH.
H1v / 25A13: Renal handling of glucose
Glucose = dietary monosaccharide used for aerobic metabolism
Glycosuria = excretion of glucose in urine → pathological
Renal Handling
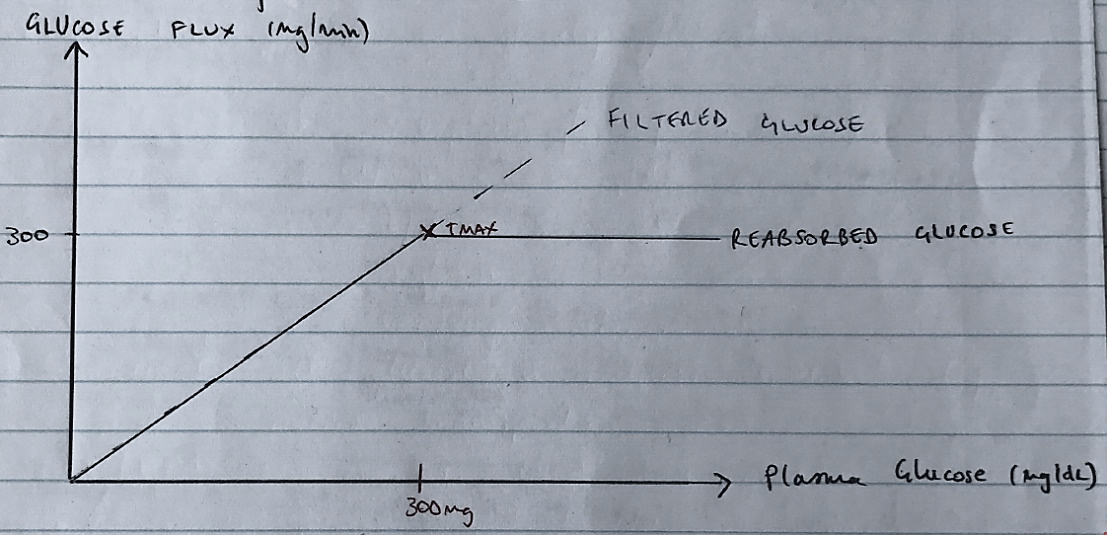
Filtration: glucose is freely filtered
Filtered glucose = GFR x [plasma glucose]
= 125mL/min x 80mg/dL
= 12.5dL/min x 80mg/dL
= 100mg/min
Reabsorption: all glucose is completely reabsorbed by active transport
Na/K/ATPase creates electrochem gradient on BL membrane (active transport)
SGLUT carries glucose coupled to Na= on apical membrane (2nd active transport)