22B08: Exam Report
Classify calcium channel blockers providing examples (15% marks). Describe the pharmacology of verapamil (85% marks)
35% of candidates passed this question.
Most candidates provided an acceptable classification of calcium channel blockers. Candidates are encouraged to read the question as a few failed to provide relevant examples with their classification.
A basic understanding of the common features of verapamil (indeed most of these are common to the calcium channel blockers as a group) in clinical practice and toxicology was sufficient to pass.
Marks allocated to dosing and presentation were not gained for writing that it is available as tablets or as a clear colourless solution, unless relevant information was given.
Many candidates listed neuropsychiatric effects of verapamil, which are not a feature normally associated with calcium channel blockers.
Many also listed QT prolongation among its effects, which is not listed in the standard texts and is the opposite to the true effect.
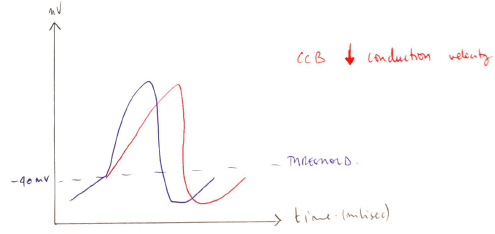
The examiners noted that in some papers there appeared to be a contradiction between the effect of Verapamil on the cardiac action potential and the detail provided about the drugs clinical effects, these answers demonstrated a lack of solidity in the understanding of the underlying physiology.
14A02: Exam Report
Classify calcium channel blockers, and give an example for each classification. (30% of marks) Describe the pharmacology of verapamil. (70% of marks)
61% of candidates passed this question.
Most candidates managed to provide a classification of calcium anatagonists.
The pharmacology of verapamil was less well understood. The structure for answering a pharmacology question was often poor and there was commonly a lack of precision in pharmacokinetics.
We suggest that candidates look at a general pharmacokinetic structure when answering these questions. One approach would be a structure that covers drug name and description, pharmaceutics (chemistry / ampoule contents), Pharmacokinetics, Pharmacodynamics (Think CNS / CVS / Resp/GIT etc. if relevant), Dose and Side effects then Indications and Contraindications can help organize the information.
G7iii / 22B08 / 14A02: Classify CCB. Pharmacolgy of Verapamil
Calcium Channel Blockers
- Class 4 antiarrhythmics
- Diverse & structurally unrelated
- All block Ca2+ channels
- Classified on basis of CHEMICAL STRUCTURE
Dihydropyridines → Nimodipine
- Block Ca2+ channel of peripheral arteries
- Via extracellular modulation of Ca2+ channel
- Prevents Ca2+ entry into smooth m. cell
Benzothiapines → Diltiazem
- Intermediate between the other 2
- Predominate effect = AV NODE
- Inhibits inward Ca2+ current
- ↓rate conduction of AV Node → ↑PR interval
Phenylalkylamines → Verapamil
- Predominant AV Node, SA Node
- Physically occludes Ca2+ channel
- ↓rate conduction → ↑PR interval
Verapamil
Verapamil
Chemical
Synthetic papaverine derivative
Use
- Hypertension
- Angina
- SVT
Presentation
Tablets
Racemic mixture → solution for injection
L isomer = inhibits Ca2+ influx across slow (L type) Ca2+ channels
D isomer = no Ca2+ blocking activity; mimics LA at fast Na+ channels
Dose
PO: 250 – 480mg (divided doses)
IV: 5 – 10mg over 30 sec
→ PO dose much higher than IV dose due to extensive 1st pass metabolism
Route
PO: 240 – 480mg
IV: 5 – 10mg → then can infuse 5mcg/kg/min to sustain effect
Onset
IV peak effect 3 mins
DoA
20 mins
MoA
- Competitive antagonist at L-type Ca2+ channels
- ↓Ca2+ influx into vascular smooth m. & myocytes
- Inhibits contraction
Verapamil’s predominant effect is at AV node, but also SA node, myocardium, peripheral vessels
PD
CVS:
- Class & antiarrhythmic
- ↓automaticity (↓Ph 4 depolarisation)
- ↓conduction velocity
- ↑refractory period
- AV conduction slowed
- – ve inotrope
- Vasodilation arterioles → ↓BP
- Potent CA vasodilation
CNS: Cerebral vasodilation
GU: ↑RBF 2° ↓ vascular resistance
PK
A
20% OBA
Significant 1st pass
D
>90% PPB (all CCBs)
VD 5L/kg
M
Demethylation & dealkylation in liver
Norverapamil = activity
E
70% metabolites excreted in urine
16% metabolites excreted in faeces
t ½ B 6hrs
Adverse Effects
- Hypotension
- Profound -ve inotropy with overdose
Multiple drug interactions
- Potentiate NMBD
- Volatiles → -ve inotropy
- ↑risk LA toxicity with verapamil
- ↑[Digoxin] levels ∴↑ risk toxicity
- Huge additive -ve chrono & inotropic effect in conjunction with β blockers