PARACETAMOL TOXICITY
Toxicity = the degree to which something is poisonous
· Paracetamol therapeutic range = 10 – 20mcg/mL
· Toxicity occurs if >10g ingested/24hrs
Metabolised by 2 pathways
1. 90% metabolised to glucuronide & sulphate
2. 10% metabolised by CYP450 to NAPQI → then conjugated to glutathione
Mechanism of toxicity
· ↑NAPQI levels
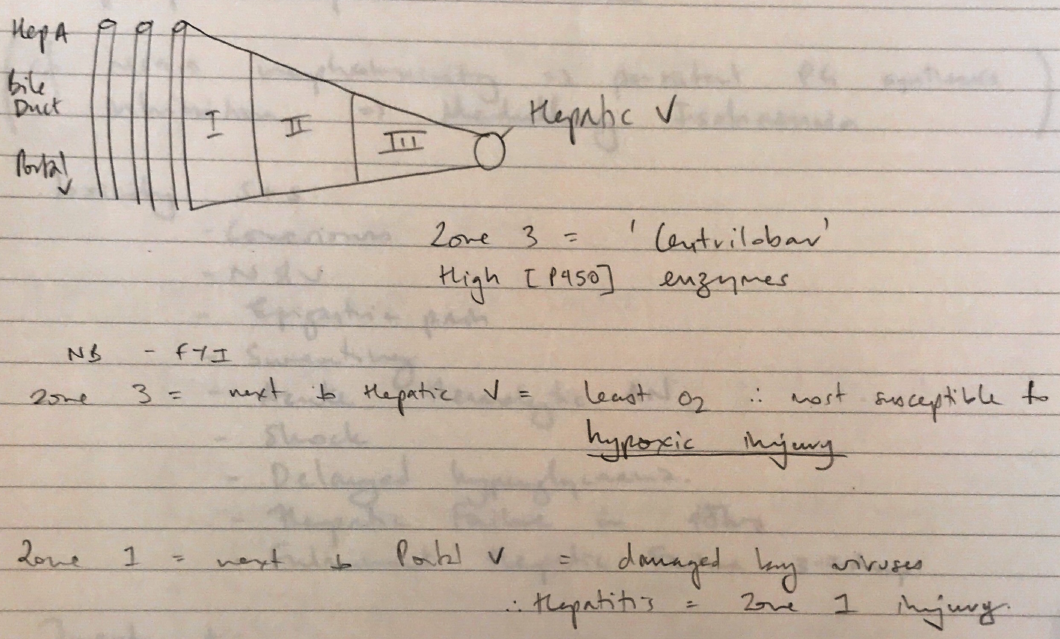
· Forms covalent bonds with sulphadryl groups on hepatocytes → cell death → centrilobular necrosis
4 mechanisms of liver damage
1. Excess paracetamol
2. Excess CYP261 activity → inducers (phenytoin; rifampicin)
3. ↓ capacity to metabolise to glucuronide/sulphate
4. ↓ glutathione stores
When NAPQI reacts with hepatocytes = IRREVERSIBLE INJURY
Nephrotoxicity
· Metabolite p-aminophenol accumulates in renal papillae
· Causes necrosis because binds covalently to sulphydryl groups & depletes glutathione
Cf. NSAID nephrotoxicity → persistent PG synthesis inhibition → medullary ischaemia
Toxicity S+S
· N&V
· Epigastric pain
· Sweating
· Acute haemolytic AN
· Shock
· Delayed hyperglycaemia
· Hepatic failure in 48hrs
· Fulminant hepatic failure 3 – 7 days
TREATMENT
· Activated charcoal in 4hrs
· ABC, IV glucose
· NAC → metabolized to glutathione which can conjugate with NAPQI
· Treatment based on normogran (Rumack-Mathew)