Xi / 21B08 / 17B23 / 14A18: Anatomy of the internal jugular vein
21B08: Exam Report
Describe the anatomy of the internal jugular vein including surface anatomy landmarks relevant to central venous line insertion
38% of candidates passed this question.
The overall pass rate for this question was poor considering how relevant this area of anatomy is in our daily practice. Better scoring answers used a template including a general description, origin, course and relations, tributaries and as requested in this question, the surface anatomy. Many answers that scored poorly only provided the briefest detail, were vague in their descriptions and incorrect with respect to the facts presented or imprecise with respect to the terminology used.
17B23: Exam Report
Outline the anatomy of the internal jugular vein relevant to central venous line cannulation (80% of marks). Include important anatomical variations (20% of marks).
14% of candidates passed this question.
Good answers were structured including origin, termination, tributaries, relationships, surface anatomy and common variations.
Factual inaccuracies were common and there was confusion about the relations of the internal jugular vein. Many candidates did not mention the changing relationship between the internal jugular and the carotid artery as they travel through the neck or the changes that result from repositioning for insertion. Many candidates also forgot to mention surface anatomy and a number talked about ultrasound and views used for insertion of central lines. Common omissions included the origin, tributaries, relationship with the correct cranial nerves and the fact that it is usually larger on the right. Almost nobody mentioned the relationship to the pleura.
14A18: Exam Report
Outline the anatomy of the internal jugular vein. (80% of marks) Describe the Doppler Effect. (20% of marks)
40% of candidates passed this question.
An overview of the Internal Jugular vein stating where it is formed and terminates would be a good start. The important surface anatomy of the vein (left and right) followed by mention of the important anatomical relationships was then required. Few candidates mentioned anatomical variations.
Many answers had no identifiable structure and went back and forth around the topic as information came to mind. A number of answers contained very rough diagrams that did not contain mark worthy information but took time to draw.
The second part of the question was generally well answered by those attempting it. Many candidates ignored or forgot about this part of the question. Some candidates wrote 2 or more pages of significant detail in stark contrast to what they had written for the first part of the question. The percentage of marks allocated is a good guide as to the level of detail required in the answer.
Xiii / 21B08 / 17B23 / 14A11: Outline the anatomy of the internal jugular vein
Anatomy
Origin
- Originates at jugular bulb(dilation formed by confluence of inferior petrosal sinus & sigmoid sinus)
- Exits skull via jugular foramen
- Usually larger on right
Course
- Starts superior bulb of IJV
- Lies posterior to internal carotid artery with glossopharyngeal (CN IX), vagus (X), accessory (CN XI), hypoglossal (CN XII) nerves passing between their adjoining surfaces
- Descends laterally to internal carotid (& later common carotid) in carotid sheath (superficial in anterior triangle of neck)
- Descends deep to sternocleidomastoid muscle
- Inferior bulb → terminates behind sternal end of clavicle, where it joins with subclavian veinto form brachiocephalic vein
- Head → Chest (Posterior to internal carotid → Lateral to common carotid → Anterolateral)
Borders
- Anterior: SCM
- Posterior (from superior to inferior): Lateral mass of C1, scalene muscles, lung pleura, sympathetic chain
- Medial: Internal carotid & common carotid, 4 cranial nerves (glossopharyngeal, vagus, accessory, hypoglossal)
Relationships
- Vagus nerve lies behind/between carotid & IJV
- Cervical sympathetic plexus lies posterior to carotid sheath
- Deep cervical lymph nodes lie close to vein
- External jugular crosses sternomastoid belly of SCM, running posteriorly & more superficial to IJV later perforating deep fascia to drain into subclavian vein
- Pleural rises above clavicle 2.5cm, close to the vein at its termination
- Thoracic duct passes lateral to confluence of left IJV and SCV, may be injured during leftIJV cannulation
- Right lymphatic duct may be injured during right IJV cannulation (less common due to smaller size)
Tributaries
- Inferior petrosal sinus
- Facial, pharyngeal, lingual, superior thyroid, middle thyroid, occipital veins
Relation to Carotid
- C2: Posterior
- C3: Posterolateral
- C4: Lateral
Anatomical Variants
- Posterior/medial positions of IJV in relation to carotid artery
- Superior vena caval duplication – IJ enters persistent left sided SVC
- IJ duplication: Bifurcation of the vein with each branch having a separate connection to the subclavian vein
- IJ fenestration: Bifurcation that reunites proximal to the subclavian vein
Surface Anatomy
Identify triangle formed by 2 heads of SCM & clavicle
Palpate artery and ensure site of entry is lateral to carotid
- Caudally at 30° to frontal plane
- Parallel to sagittal plane
- Towards ipsilateral nipple
Ultrasound Anatomy
Identify vein deep to SCM
- Non-pulsatile
- Thin walled
- Compressible
Approaches
- Anterior: Medial border of SCM, 3-4cm above clavicle, requires retraction of carotid manually, aim toward ipsilateral nipple
- Central: Apex of triangle formed by each muscle belly of SCM & clavicle, 60° to skin aiming toward ipsilateral nipple (blood should be obtained within 3 cm)
- Most suitable for USS guided approach
- Posterior: Posterior edge of SCM, just superior to where EJV crosses sternomastoid, 2-3 finger breaths above clavicle, direct needle towards jugular notch (blood should be aspirated within 5cm)
Positioning
Trendelenburg position – supine with 15-30° of head down tilt → to prevent air embolus / ↑ diameter of internal jugular vein
- More important in intravascularly dry patients/non-ventilated patients
- Less important in intubated patients receiving positive pressure ventilation
- Avoid in
- Raised ICP, severe respiratory failure
- Pulmonary oedema with raised venous pressure
- Small degree of head rotation (10-20°) away from midline towards contralateral side
- Head rotation changes IJV position towards the anterior and anterolateral position
- Excessive over rotation of head and neck increases overlap of IJV over carotid artery
Mnemonic
Medical Schools Let Fun People In
- Middle thyroid vein
- Superior thyroid vein
- Lingual vein
- Facial vein
- Pharyngeal vein
- Inferior petrosal sinus
Doppler Effect
The frequency of a wave is perceived to change relative to its movement
- Used to detect & measure flow
- Positive Shift: Blood flow to transducer, reflected wave of high frequency
- Negative Shift: Blood flow away from transducer, reflected wave low frequency
- NB BART (blue away, red towards)
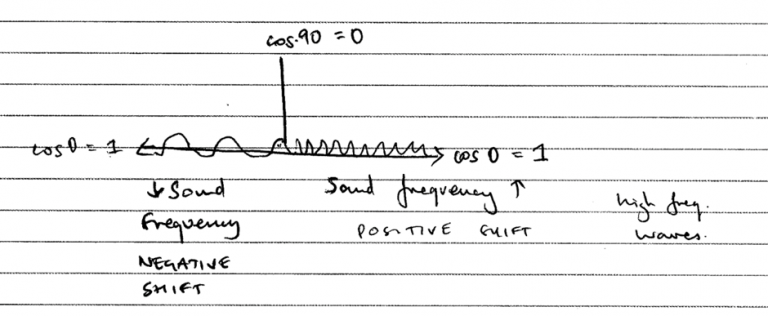
- Doppler shifts are calculated by cosine of the angle
- Maximum doppler shift @ 0 degrees (Cosine 0 = 1), flow towards transducer
- No shift if flow is perpendicular to transducer @ 90 degrees (Cosine 90 = 0)
Author: Novia Tan
- Author: Krisoula Zahariou