Define dead space and its components (15% of marks).
Describe the factors that affect each component (30% of marks).
Outline the physiological impact of increased dead space (15% of marks).
Describe methods of measurement of dead space (40% of marks).
34% of candidates passed this question.
The question structure and mark allocation is a useful guide to the level of detail required for each section.
The definition and components of dead space (apparatus, anatomical, alveolar and physiological) are relatively straightforward and were well answered.
A useful structure for this section involved a description of the factors that affect each of the components of dead space outlined in the first section. It was expected that each factor would be correlated to its effect e.g., an increase in conducting airway volume (such as in the supine position or with larger patient size) leads to increased anatomical dead space.
The major impact of increased dead space is a reduction in alveolar ventilation. Higher marks were gained by describing the consequences of this; changes in alveolar gas tension, compensatory changes in work of breathing and eventually respiratory failure once compensatory mechanisms are exhausted.
Techniques used to measure dead space are well described in both Nunn’s and West’s respiratory physiology textbooks. Anatomical dead space is measured using the Fowler’s method (nitrogen washout) and the Bohr equation with Enghoff modifications measures physiological or total dead space. Alveolar dead space is then derived by subtracting anatomical from physiological dead space. A brief description of these concepts was expected.
18A03: Exam Report
Define dead space and its components (30% of marks). Explain how these may be measured (35% of marks) and describe the physiological impact of increased dead space (35% of marks).
59% of candidates passed this question.
Some candidates failed to provide a correct definition of dead space. An outline of anatomical, alveolar and physiological dead space was expected. The Bohr equation was commonly incorrect, and many did not comment on how to measure the components of the Bohr equation. Fowler’s method was generally well described though some plotted the axes incorrectly.
The impact of increased dead space was not often well explained. Very few people stated the major impact of increased dead space is reduced minute ventilation and how this would affect CO2.
F6iv / 25B02 / 18A03: Define dead space and its components (30% of marks). Explain how these may be measured (35% of marks) and describe the physiological impact of increased dead space (35% of marks).
Definitions
Dead Space = VT that does not partake in gas exchange
V/Q = ∞
Alveolar ventilation = the effective part of VT that takes part in gas exchange
VA (alveolar ventilation) = RR (VT – VD)
Types of Dead Space
Apparatus
Anatomical
Alveolar
Physiological (anatomical + alveolar)
Apparatus Dead Space
Due to artificial breathing apparatus
Anaes. Circuit, HME filter, ETT
Anatomical Dead Space
The volume of conducting airways
150mL
Measured by Fowler’s Method (N2 washout)
Influenced by:
Age = ↑ with ↑age & infancy
Posture = 150mL sitting, 100mL supine
Neck position = ↓with flexion, ↑with extension
Drugs = ↑with bronchodilators
VT = ↑VT = ↑ because of traction on airways with large inspiration
Measured by Fowler’s method
Subject breathes through valve box
Sampling tube with rapid N2 analyser at lips
Single FiO20 inspiration
Breathes out through mouth piece
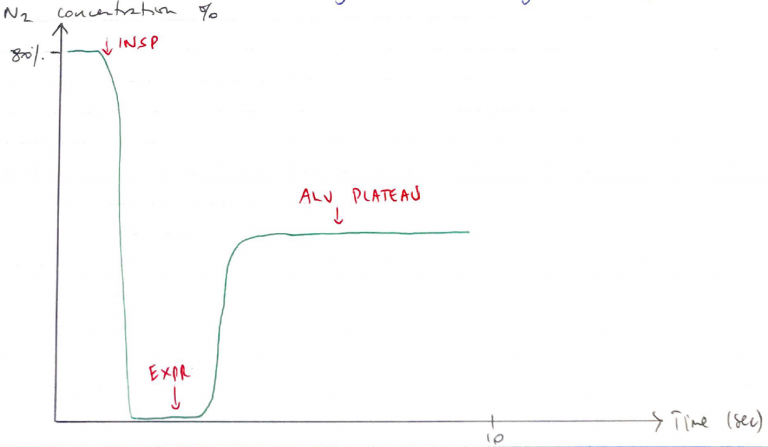
2 graphs
[N2] vs Time
3 phases
Start of expiration, no N2 because it’s measuring expired gas of conducting airways (FiO20)
N2 starts rising, because gas from alveoli starts mixing with gas from airways
Plateau → only alveolar gas being recorded
[N2] vs Expired Volume
Plot [N2] against expired volume
Draw vertical line in S so that A = B
DS is volume up to the vertical line
Alveolar Dead Space
Volume of gas reaching alveoli that doesn’t take part in gas exchange
WZ1 (PA > Pa > PV) i.e. IPPV or PE
VQ = ∞
This is pathological
Normally ~5mL
Measured by subtracting anatomical from physiological DS
Alveolar DS = Physiological – Anatomical
Physiological Dead Space
VT which does not take part in gas exchange
Physiological DS = Alveolar DS + anatomical DS
Influenced by:
Age = ↑ with ↑age
Sex = ↑with men
Posture = ↑with supine
Lung volume = ↑VT = ↑ because of traction
Pathology = PE, smoking, IPPV
Measured using BOHR EQUATION
Underlying principle that expired CO2 comes from alveolar gas, not DS units
It gives you the volume of VT that does not eliminate CO2
In health the volume derived from Bohr’s & Fowler’s methods should be similar
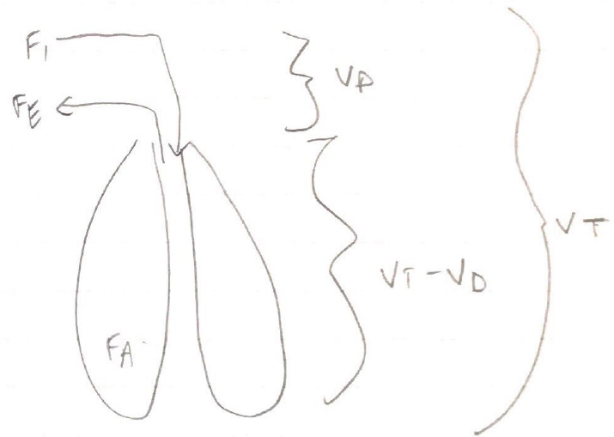
Exhaled VT = Alveolar Volume + DS Volume
Analysed for any gas i.e. CO2
Fe = expired CO2
FA = expired alveolar CO2
VT x Fe = VT x FA
VT x Fe = (VT – VD) x FA
VT x Fe = VT x FA – FA x VD
FA x VD = VT x FA – VT x Fe
FA x VD = VT(FA – Fe)
↓
The alveolar CO2 will always be higher than the CO2 in expired air
↓
Normally 1 – 5mmHg difference
Causes of ↑ Dead Space
Hypotension
PE
Artificial ventilation → preferentially pushes air to upper lung & ↑PA
Local vessel destruction
Consequences
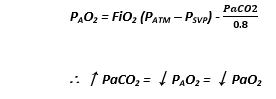
Dead space produces hypercarbia & hypoxia
Your PaCO2 will rise & your ETCO2 will fall (because remember, you’re not getting gas exchange so ↑CO2 in body + less being expired)
![[N2] vs Expired Volume](https://jennysjamjar.com.au/wp-content/uploads/2020/05/N2-vs-Expired-Volume.png)