Compare and contrast the pharmacokinetic and pharmacodynamics of IV fentanyl and IV remifentanil (60 marks). Discuss the concept of context sensitive half-time using these drugs as examples (40 marks)
66% of candidates passed this question.
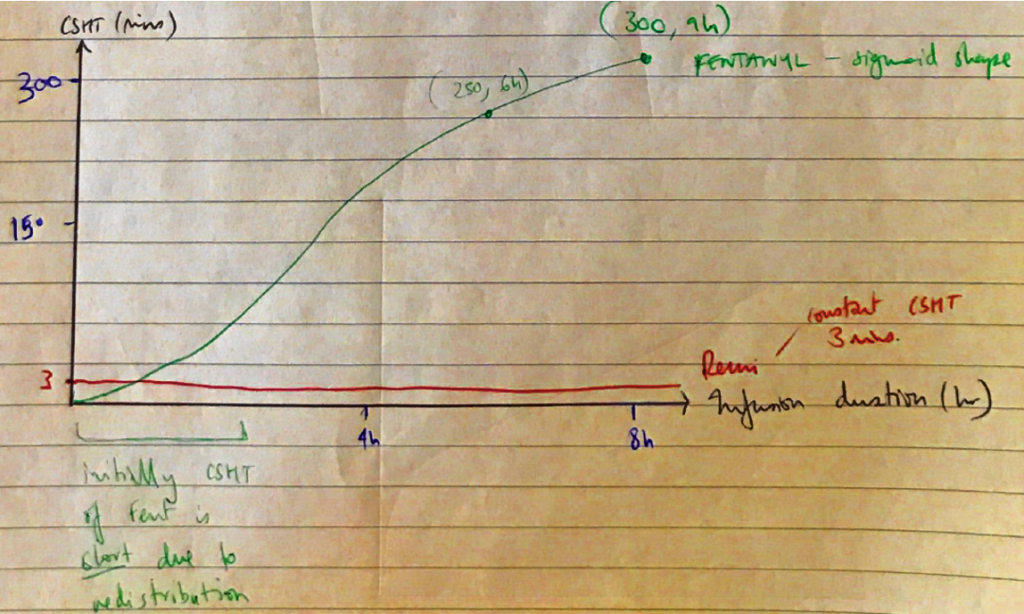
Well-constructed answers were presented in a table to compare pharmacokinetics and pharmacodynamics with a separate paragraph to discuss the concept of context sensitive half-time. Important pharmacokinetic points included: the differences in lipid solubility, ionised fractions and onset, and differences in metabolism. Marks were awarded for a definition of context-sensitive half-time. A discussion of these two drugs’ context-sensitive half-times should have included the differences in re-distribution into other compartments and rates of elimination.
Bvi / 18A05: Compare and contrast the pharmacokinetic and pharmacodynamics of IV fentanyl and IV remifentanil (60 marks). Discuss the concept of context sensitive half-time using these drugs as examples (40 marks)
Remifentanil
Fentanyl
Chemical
Remifentanil
Rapid onset, ultrashort acting Synthetic selective µ agonist of PHENYLPERIDINE CLASS
Fentanyl
Synthetic opioid of PHENYLPIPERIDINE CLASS
Rapid acting, intermediate duration
PD
Remifentanil
CNS – analgesia no effect on ICP/IOP
CVS – ↓HR, ↓BP
MSK – muscle rigidity at high dose
Immuno – no histamine release
Resp – potent resp depression
Fentanyl
CNS – Analgesia
CVS – ↓HR more common cf. M
RESP – respiratory depression most marked of all opioids. POTENT ANTITUSSIVE & chest wall rigidity
GI – less N&V
IMMUNO –histamine release
PK
Remifentanil
A
IV administration only. 100% bioavailability
D
VD 0.4L/kg
Very small
Low lipid solubility
PPB 70%
M
Rapid ester hydrolysis
Non-specific plasma & tissue esterases
Into remifentanil acid x 5000 less potent cf. remi