Describe the mechanism of action, dose and pharmacokinetics and pharmacodynamics of aminophylline
21% of candidates passed this question.
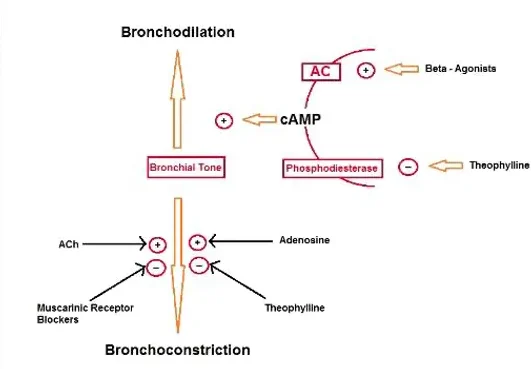
This question required a detailed description of the many mechanisms of action of aminophylline. This included PDE inhibition and the down stream pathway and its adenosine antagonist and anti- inflammatory actions.
Important pharmacokinetic concepts included hepatic metabolism with saturable kinetics and thus a narrow therapeutic window/index requiring need for drug monitoring and the risk of metabolic interactions with accelerated or reduced metabolism from inducers or inhibitors of the main enzyme (CYP1A2).
Detailed pharacodynamic consequences on the respiratory and cardiovascular systems were prioritised as well as highlighting the neurological, cardiovascular and musculoskeletal consequences of toxicity.
F1ii / 23B11: Describe the mechanism of action, dose and pharmacokinetics and pharmacodynamics of aminophylline